Building Blocks of Dermatopathology
BAD DermpathPRO Learning Hub: Basics of Immuno
Case Number : IM0006
Dr. Richard Carr
Please read the clinical history and view the images by clicking on them before you proffer your diagnosis.
Submitted Date :
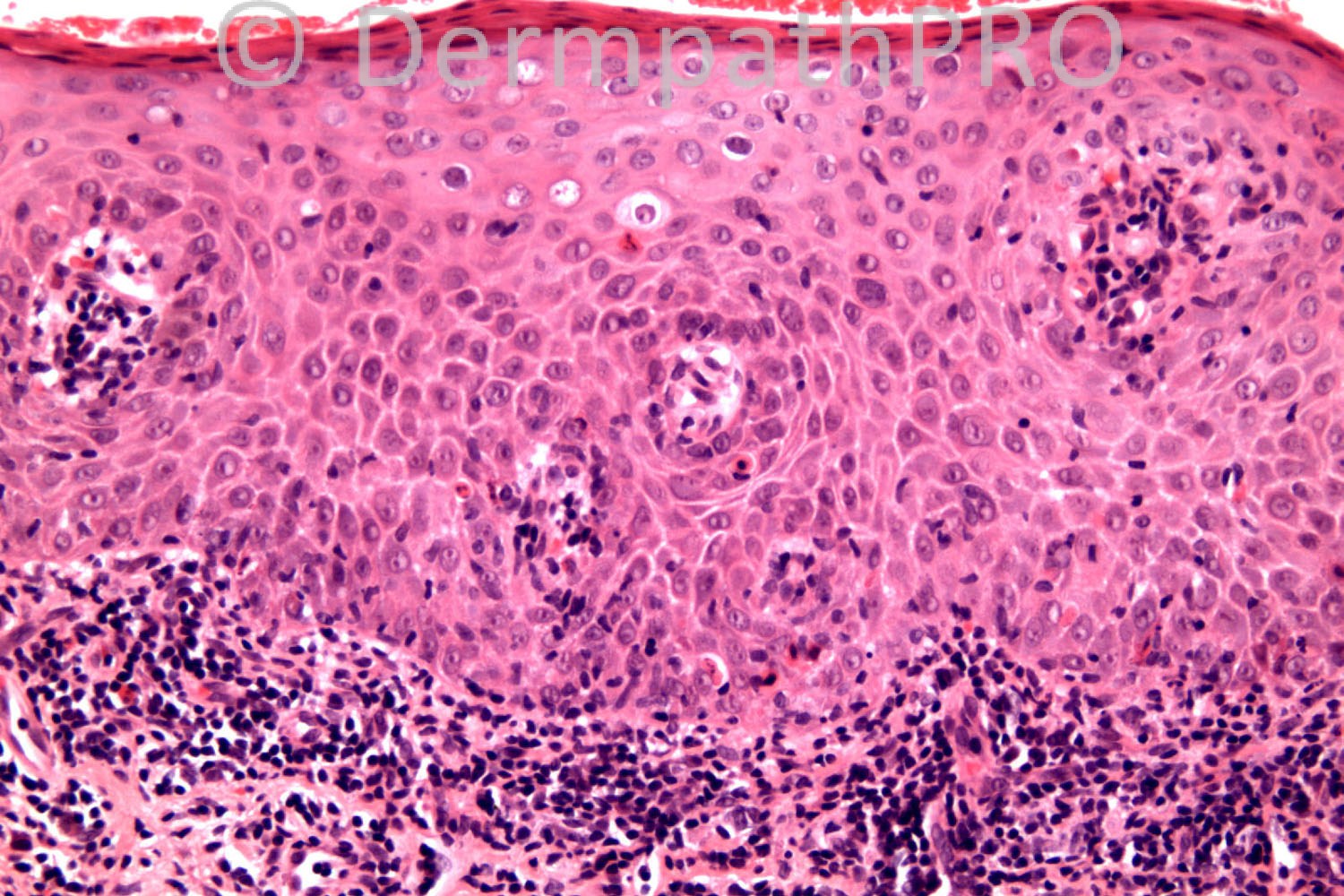
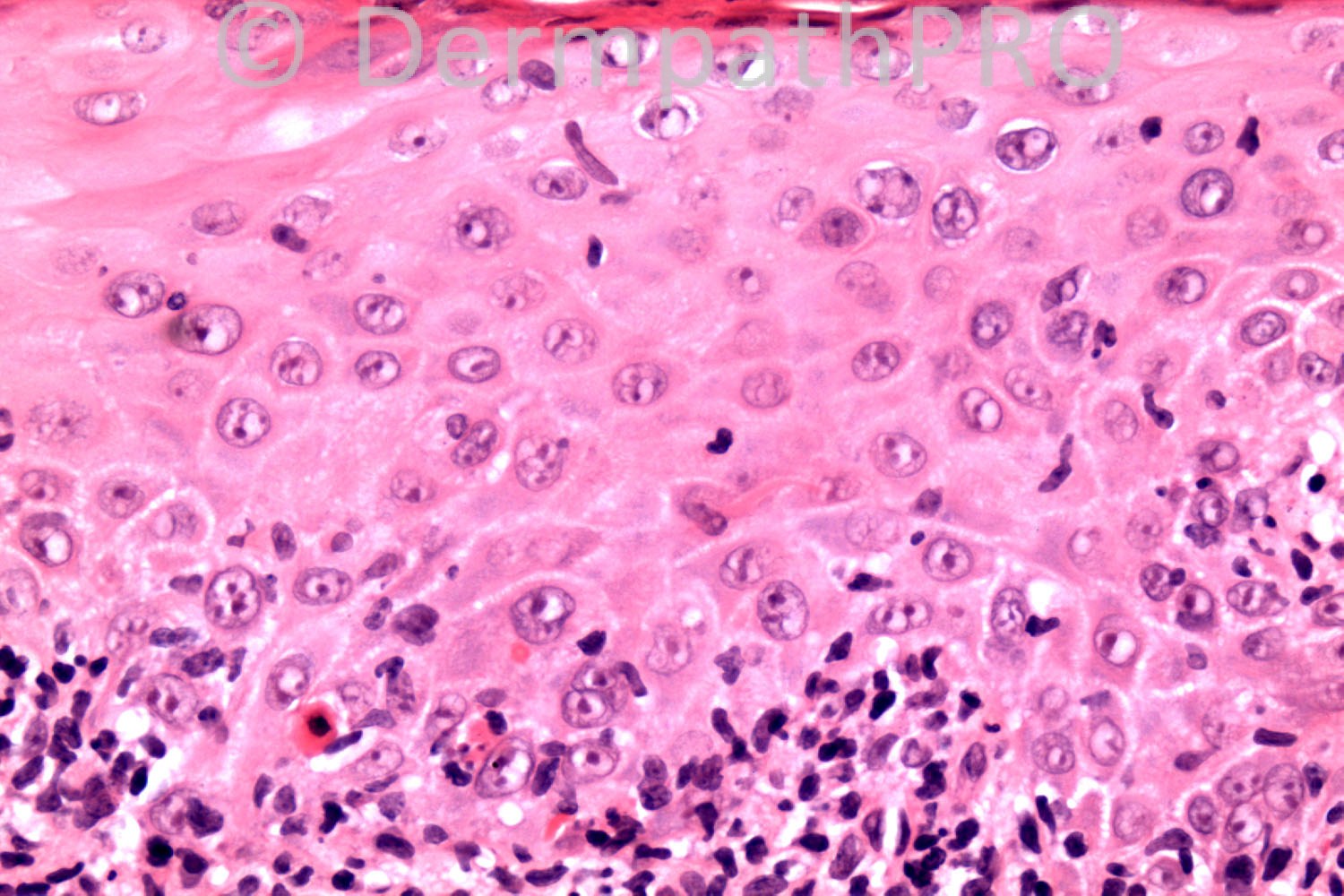
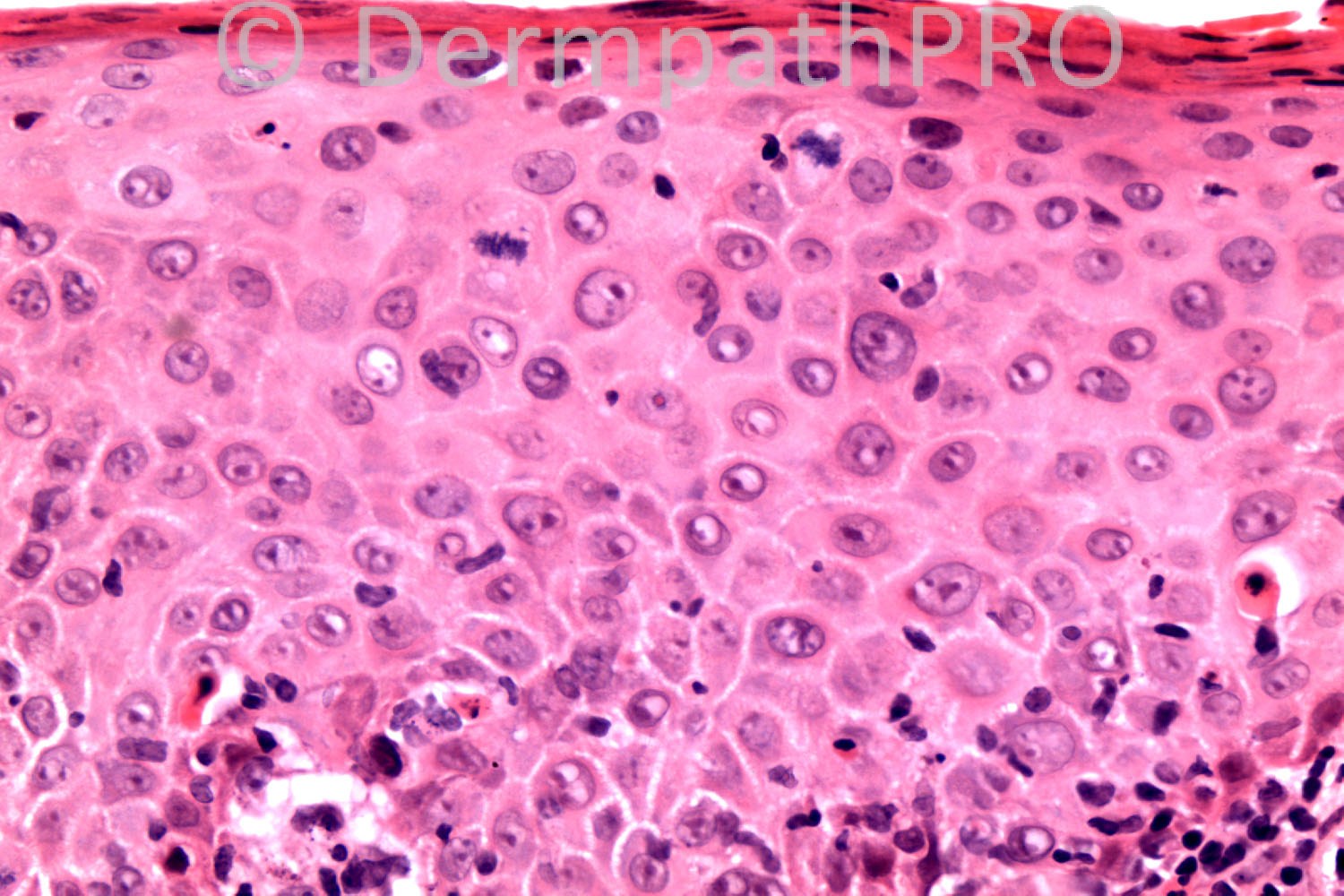
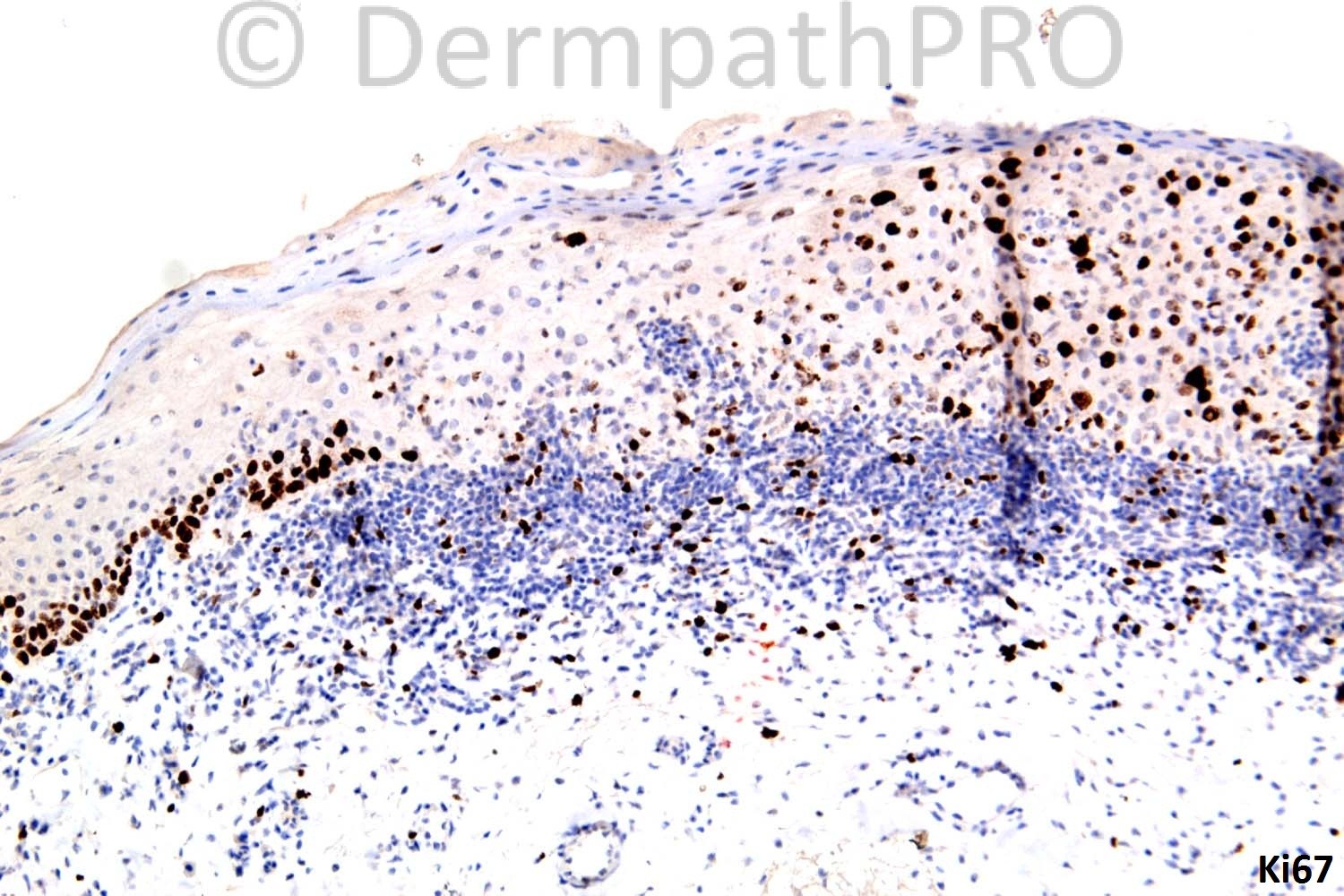
49 years-old male. Inflammatory macule ?eczema ?psoriasis.





User Feedback