Please read the clinical history and view the images by clicking on them before you proffer your diagnosis.
Submitted Date :
(0 reviews)
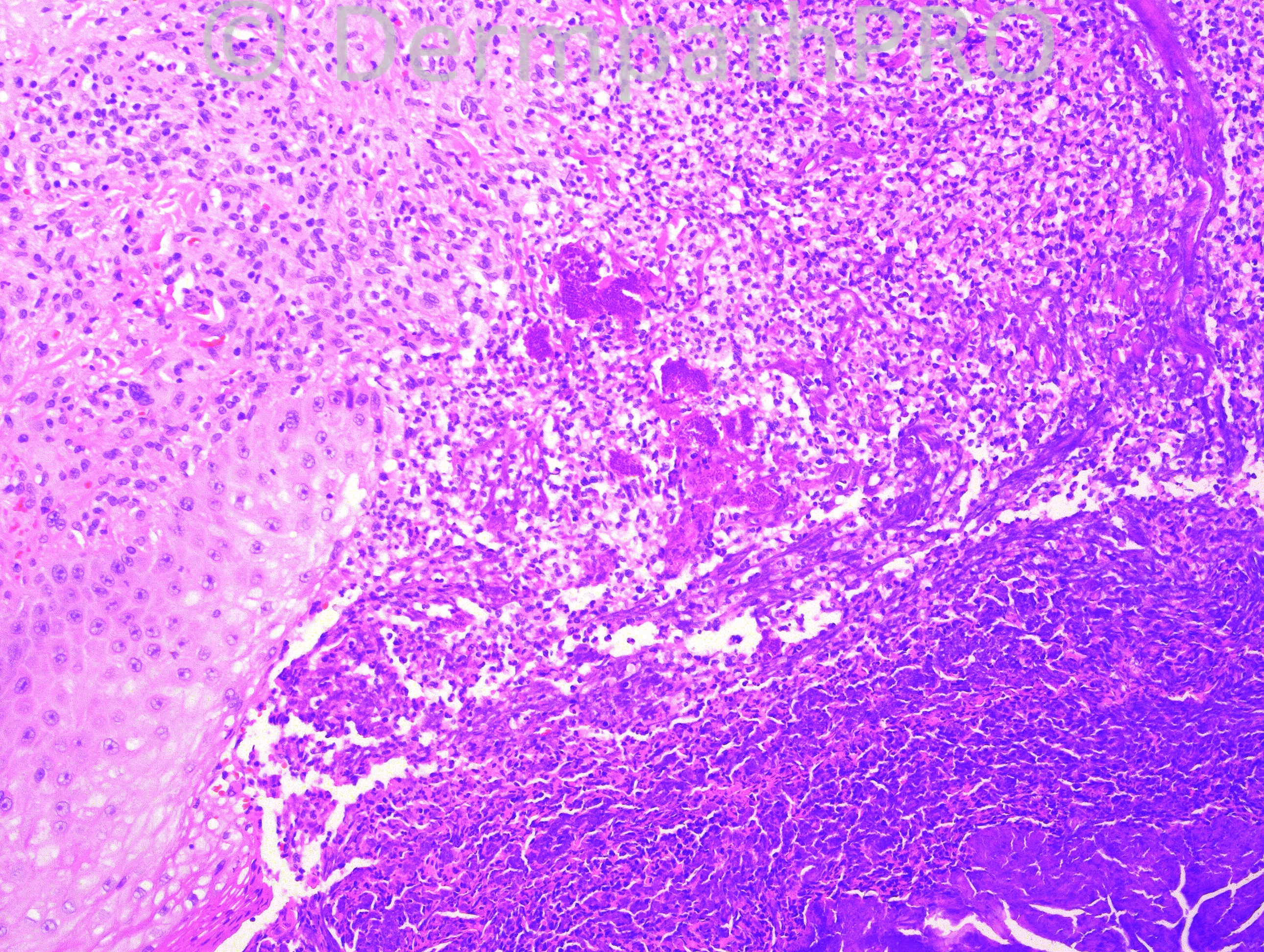
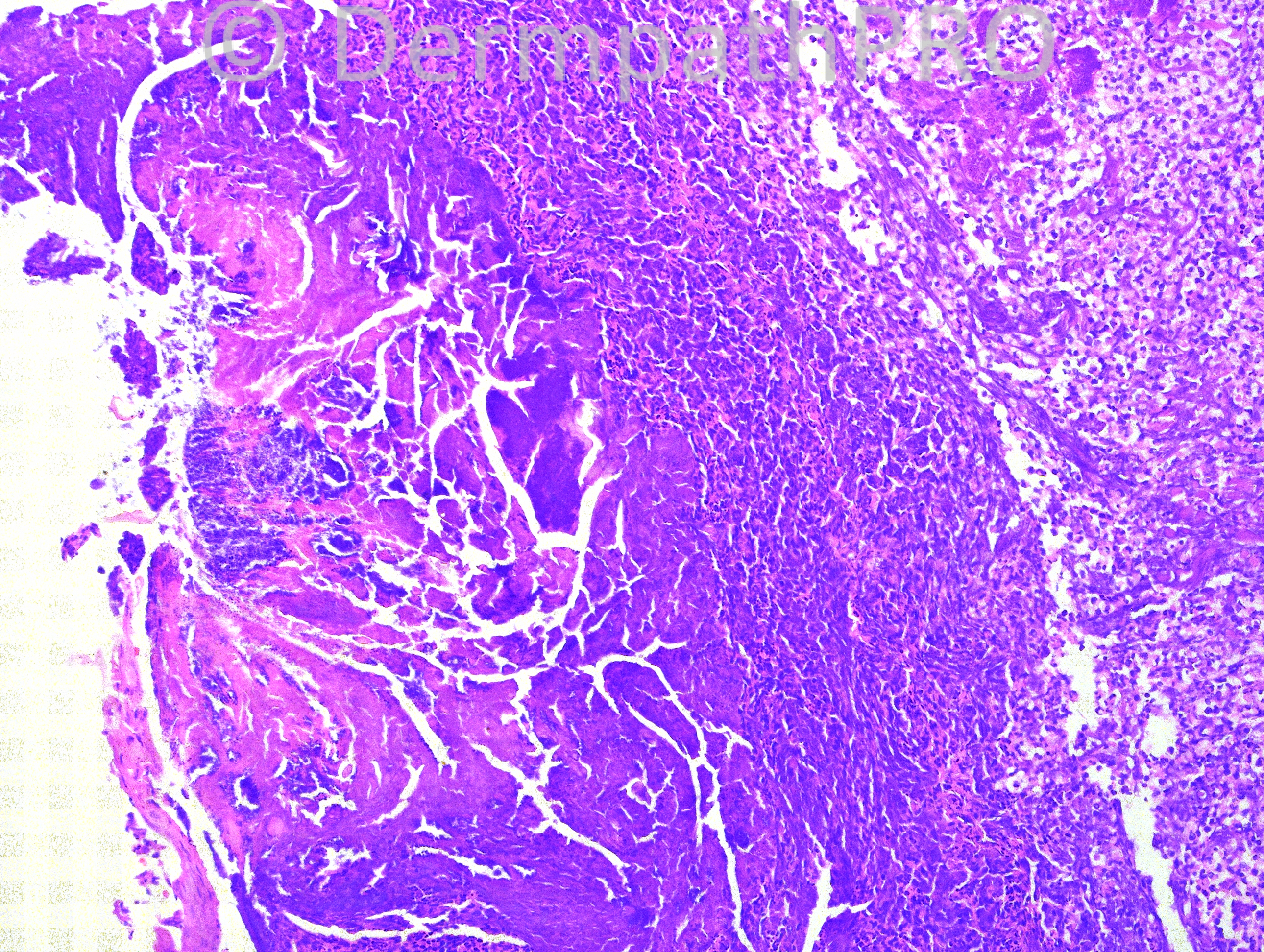
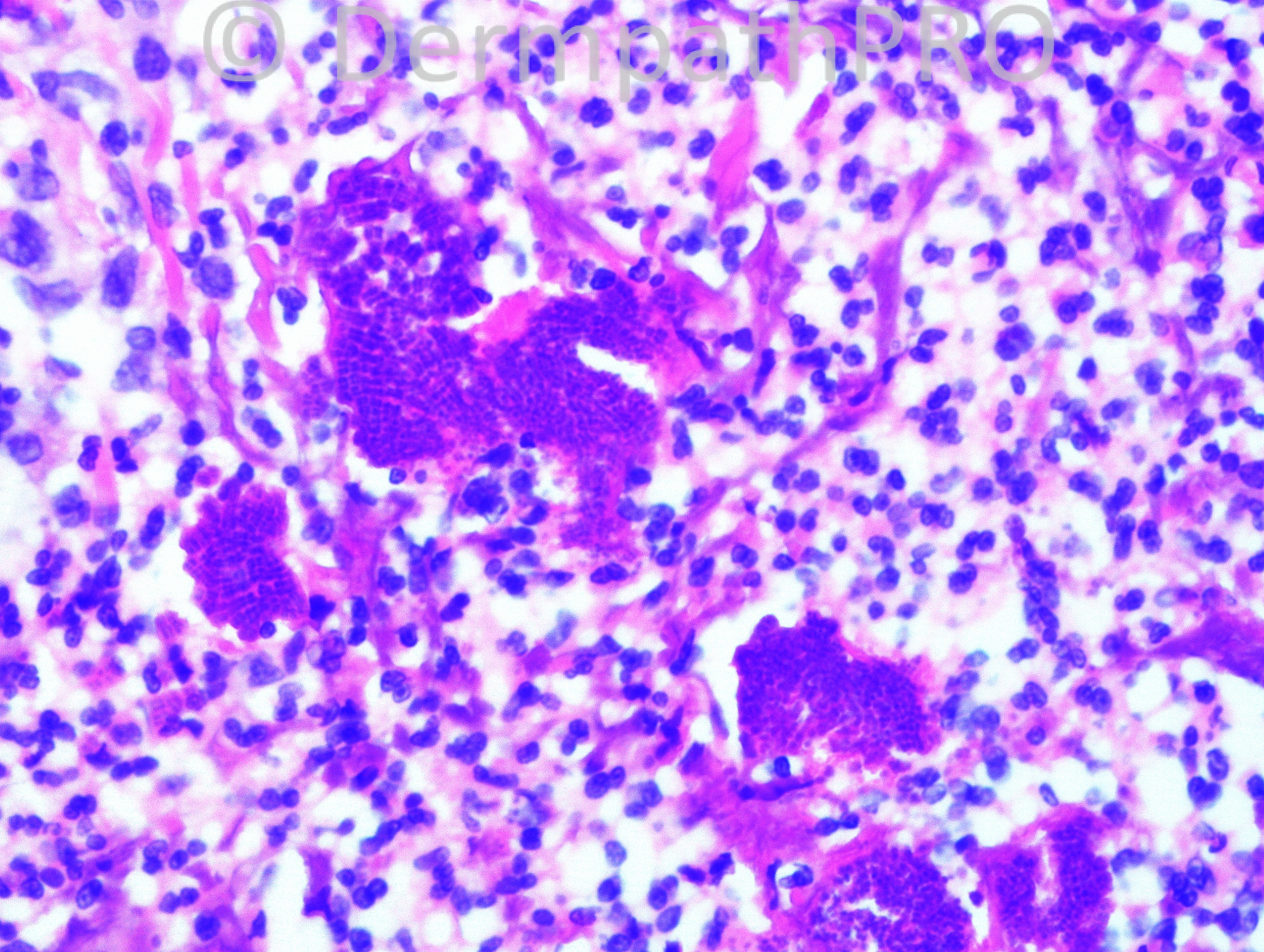
59-year-old male with recurrent papular lesion on dorsal forearm for 2-3 months. He traveled to Grand Cayman 6 months ago an to Honduras within the last 2 years. The biopsy is from an ulcerated lesion on dorsal left forearm.







User Feedback