Building Blocks of Dermatopathology
BAD DermpathPRO Learning Hub: Diagnostic Clues
Case Number : CT0005
Uma Sundram
Please read the clinical history and view the images by clicking on them before you proffer your diagnosis.
Submitted Date :
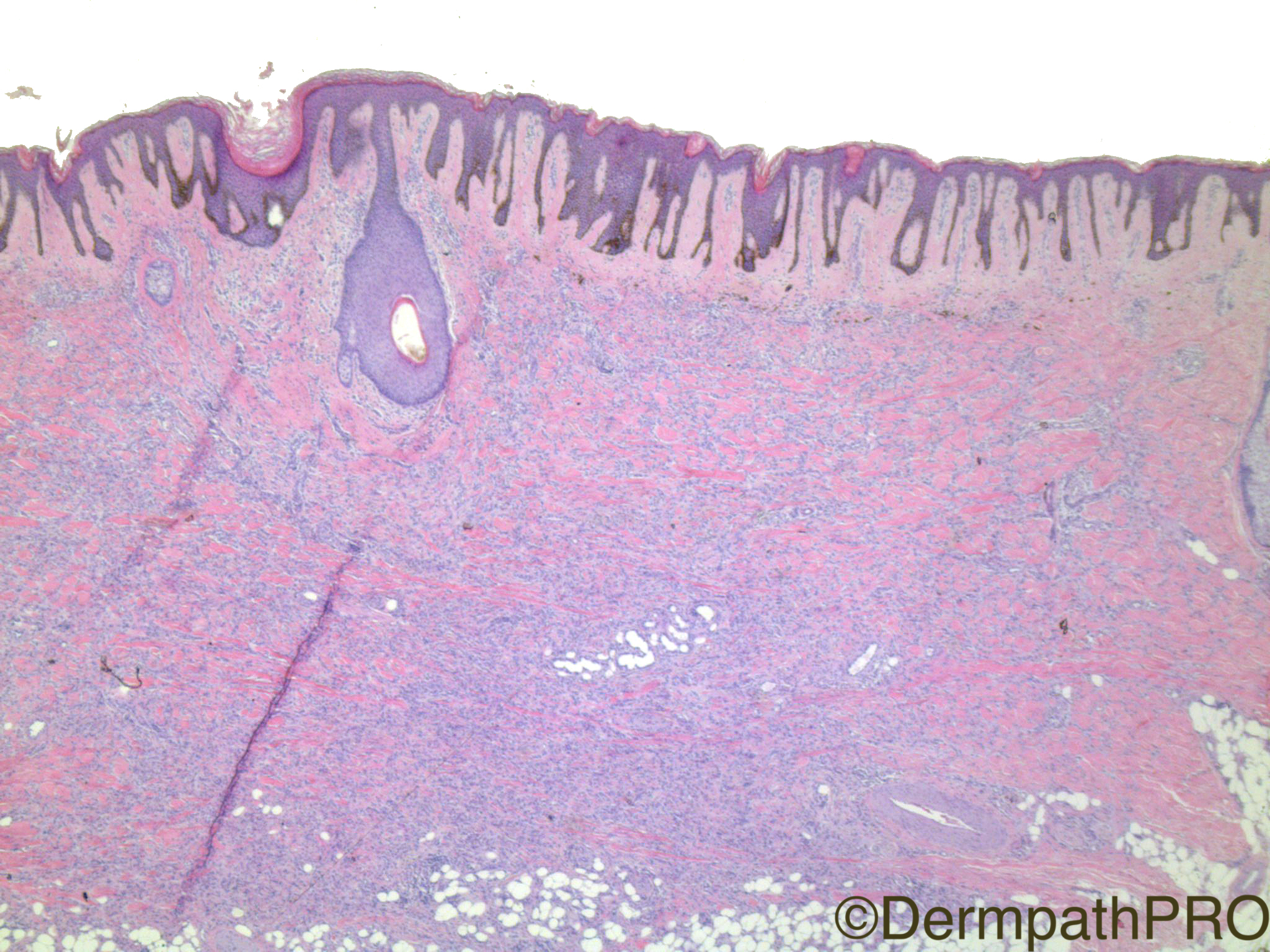
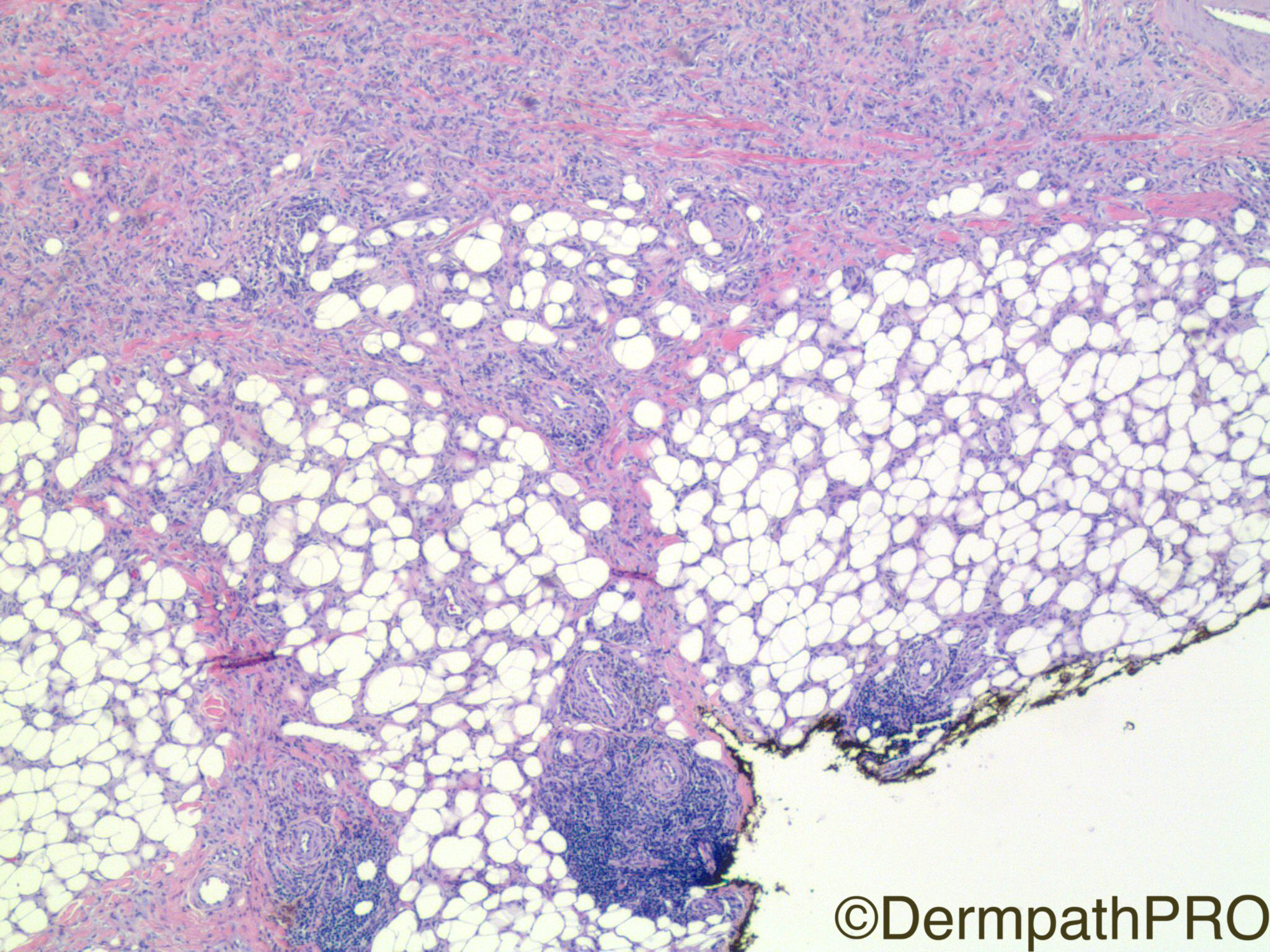
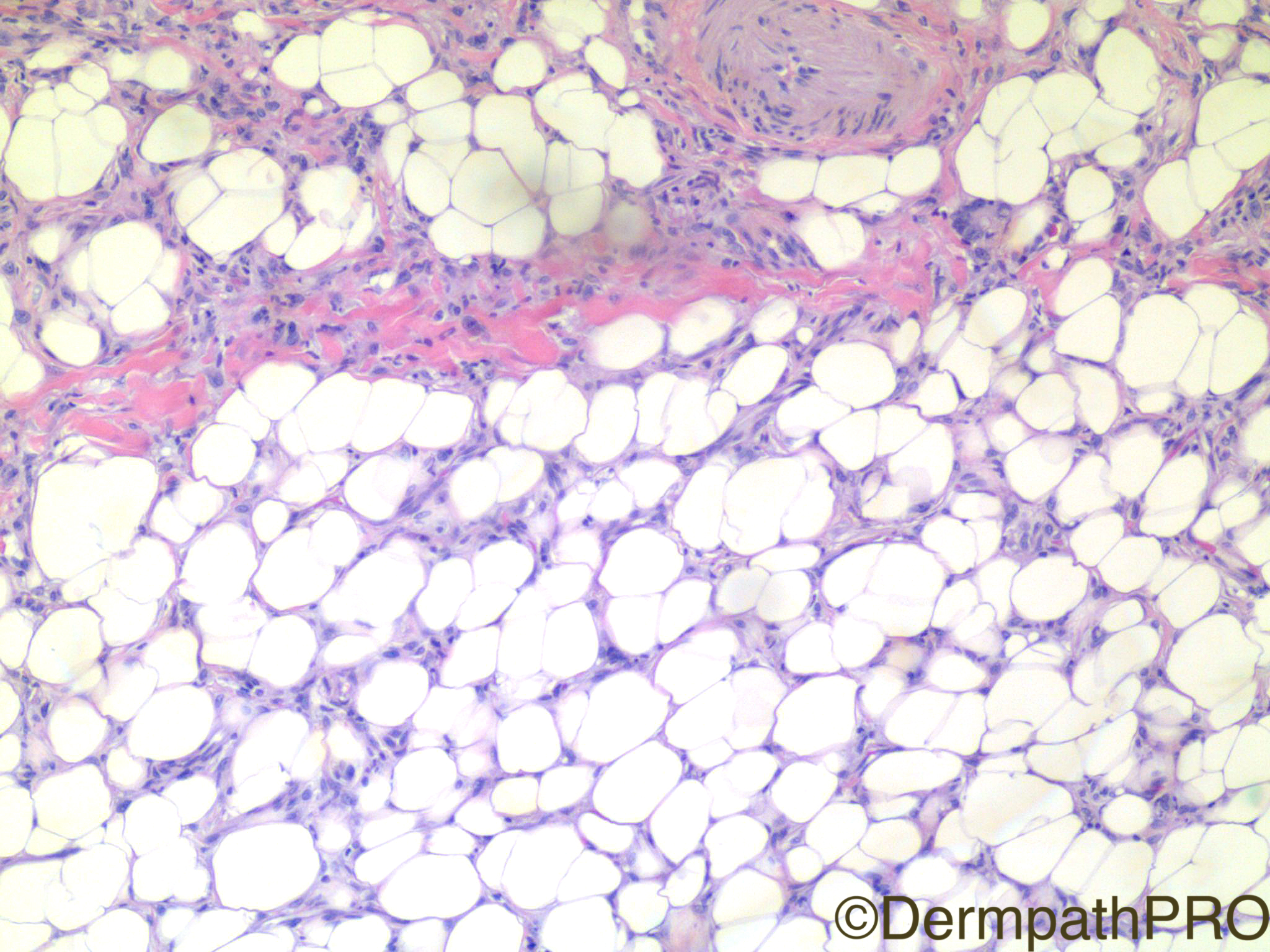
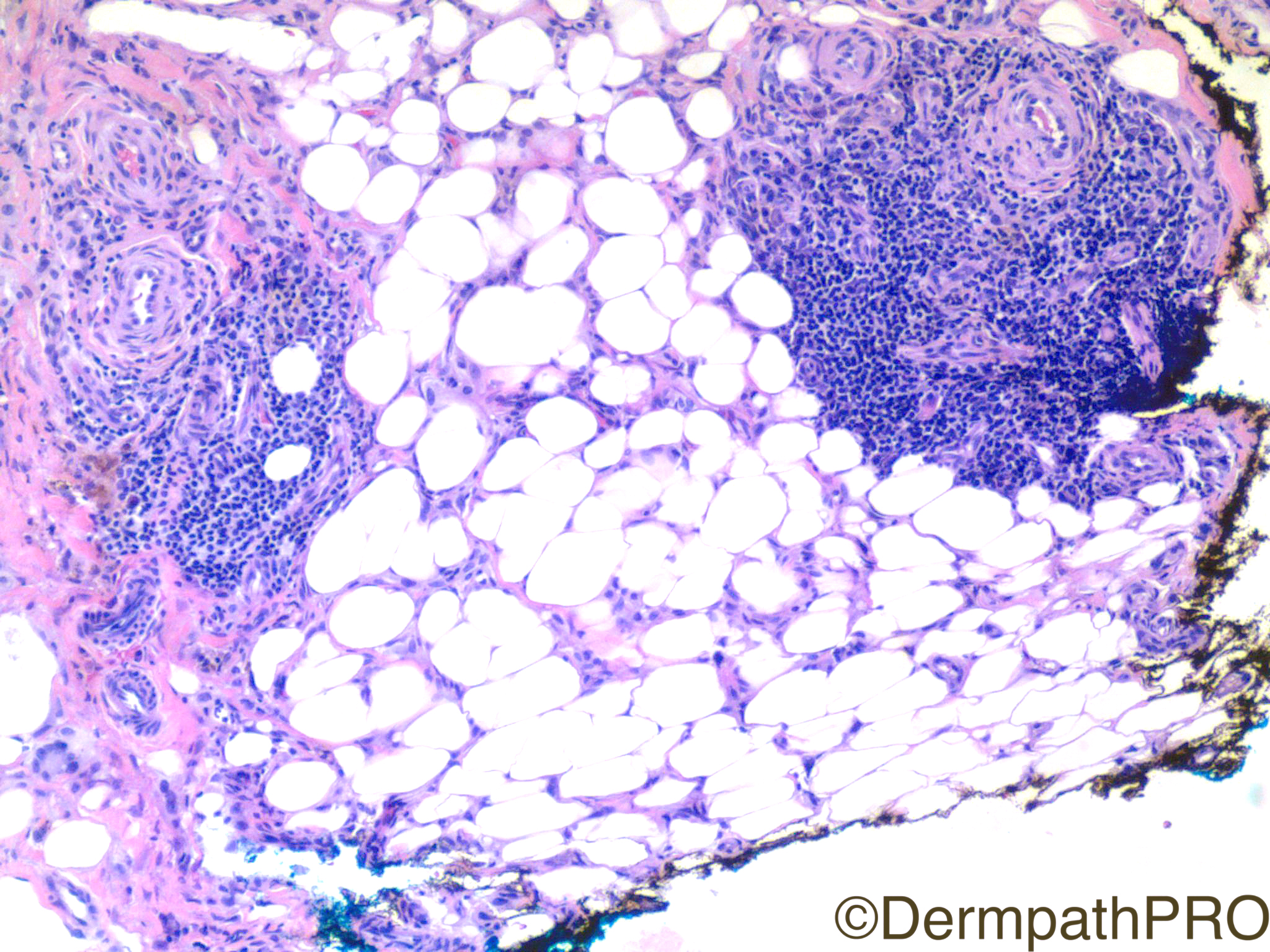
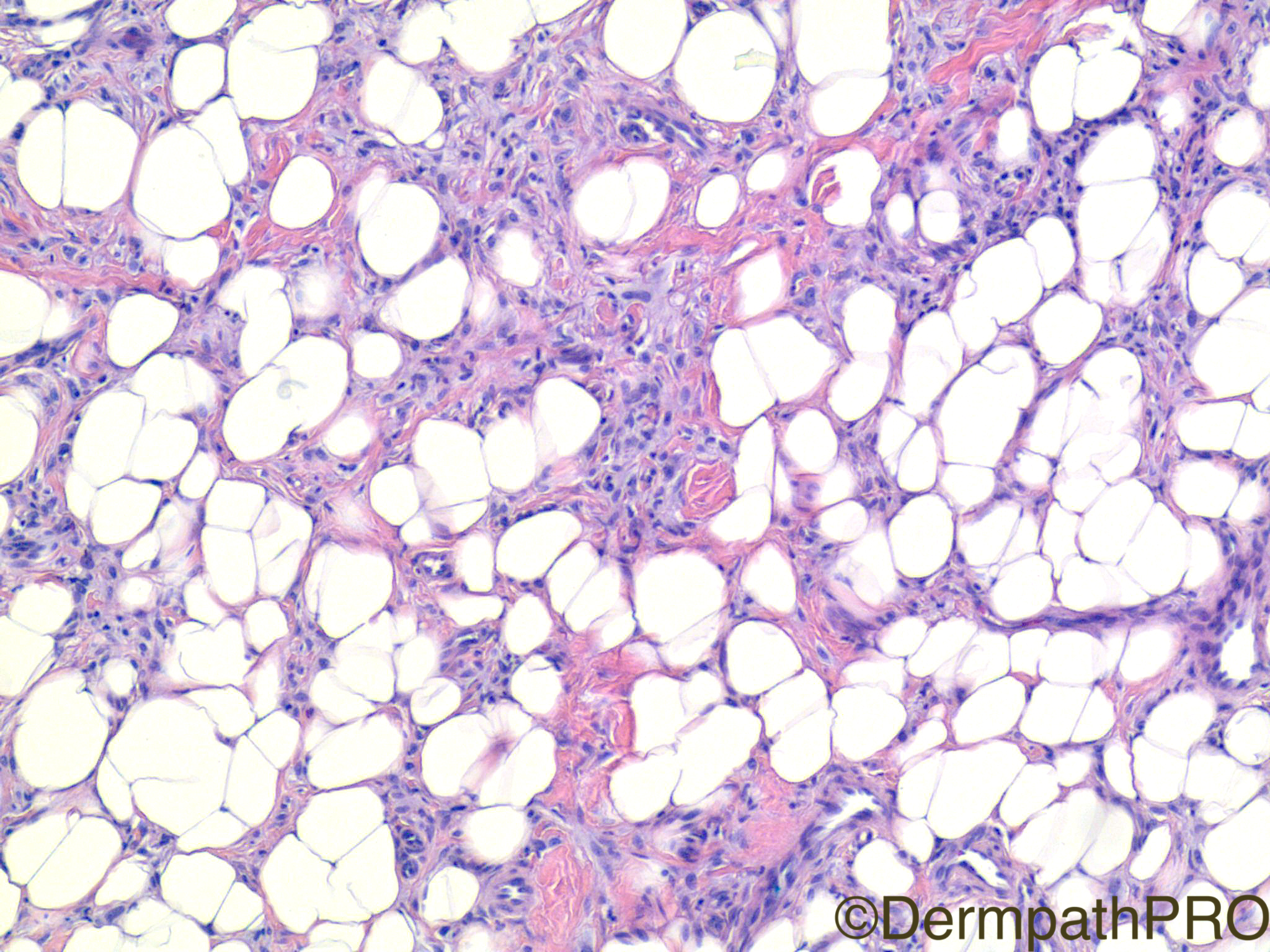
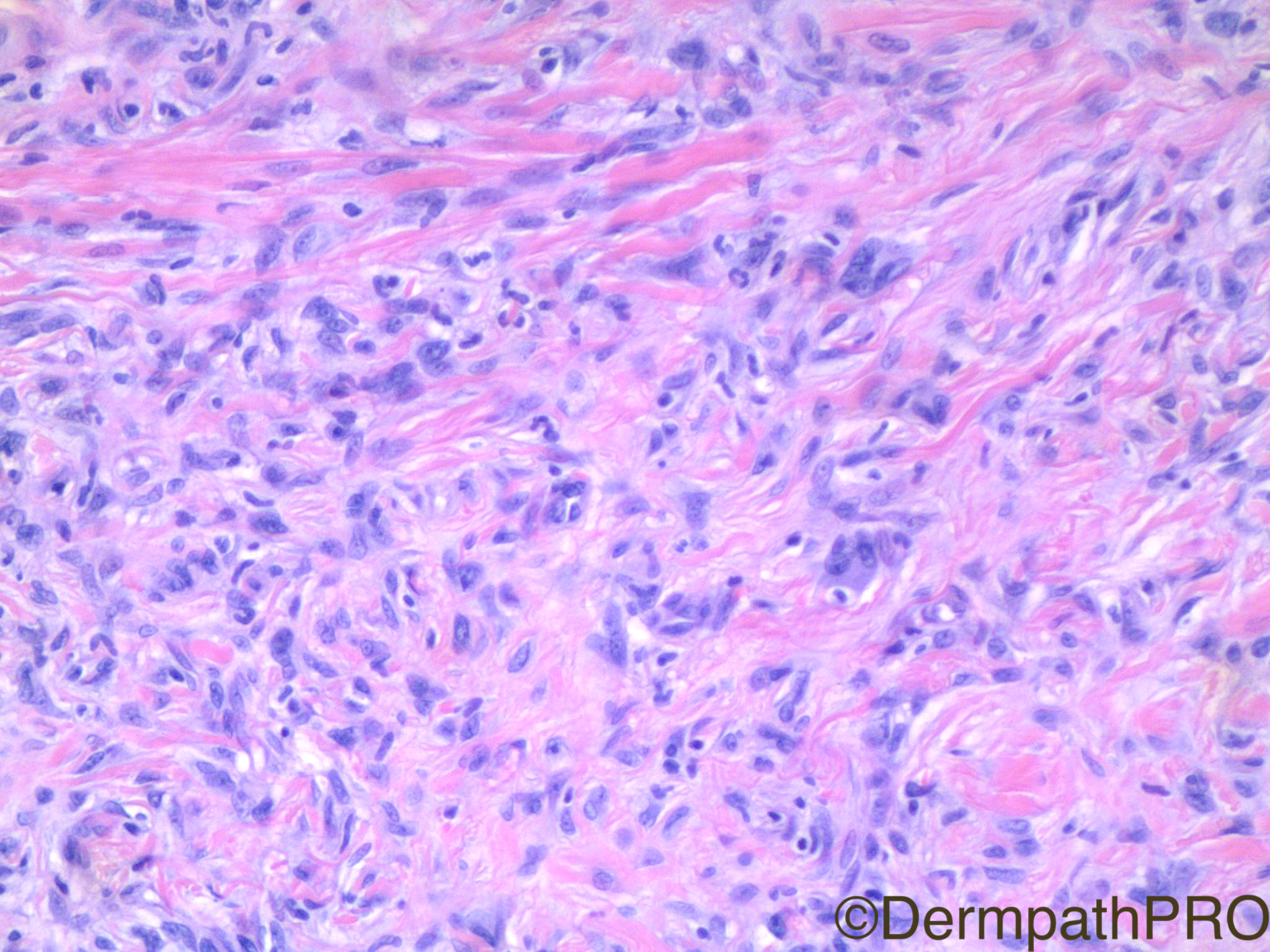
Clinical History: 49 year old woman with left anterior tibial lesion.







User Feedback