Diagnostic Pearls : CT0042
50 year old female with a shave biopsy from right upper thigh.
Posted No value





BAD DermpathPRO Learning Hub: Diagnostic Clues


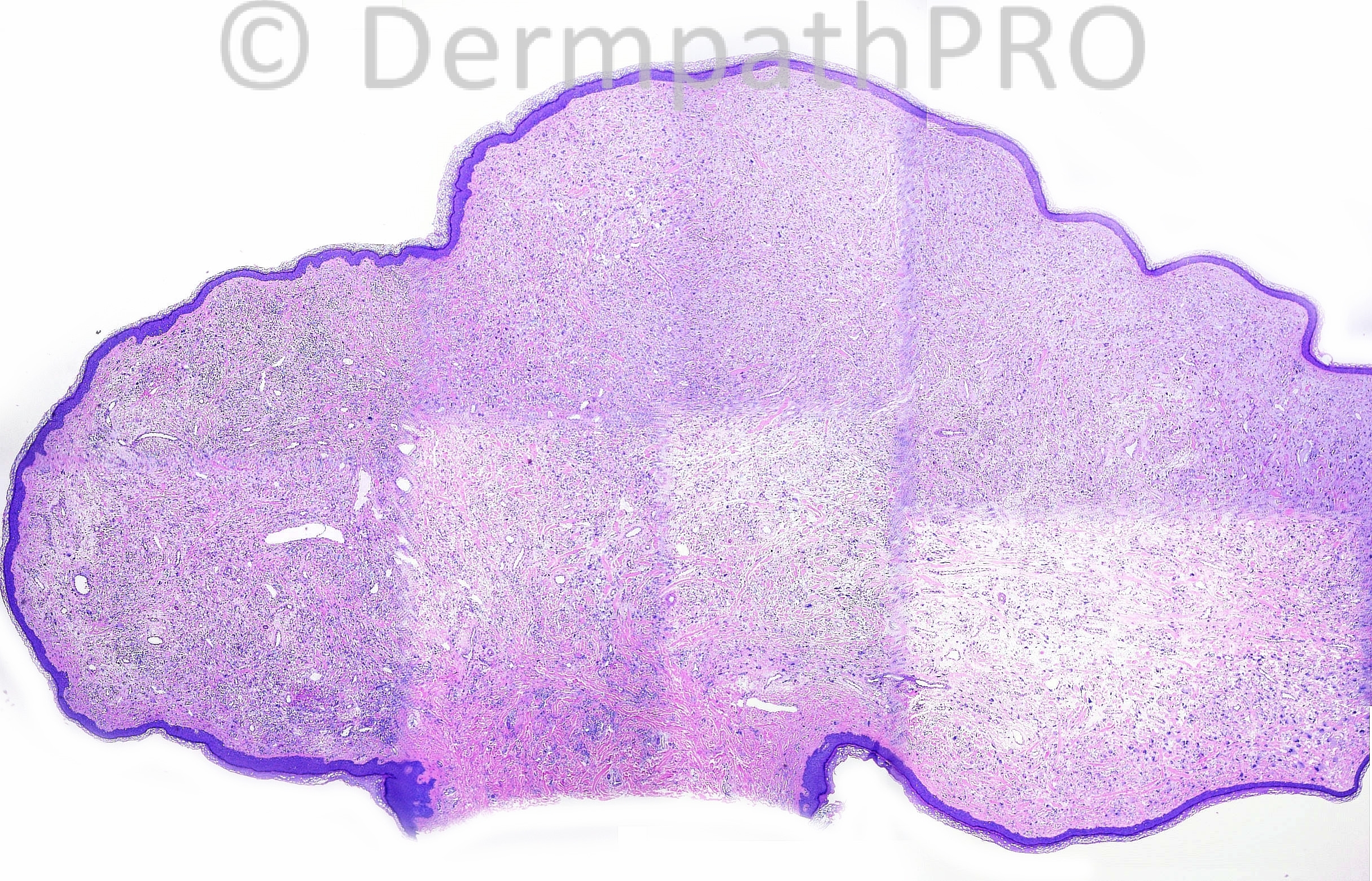
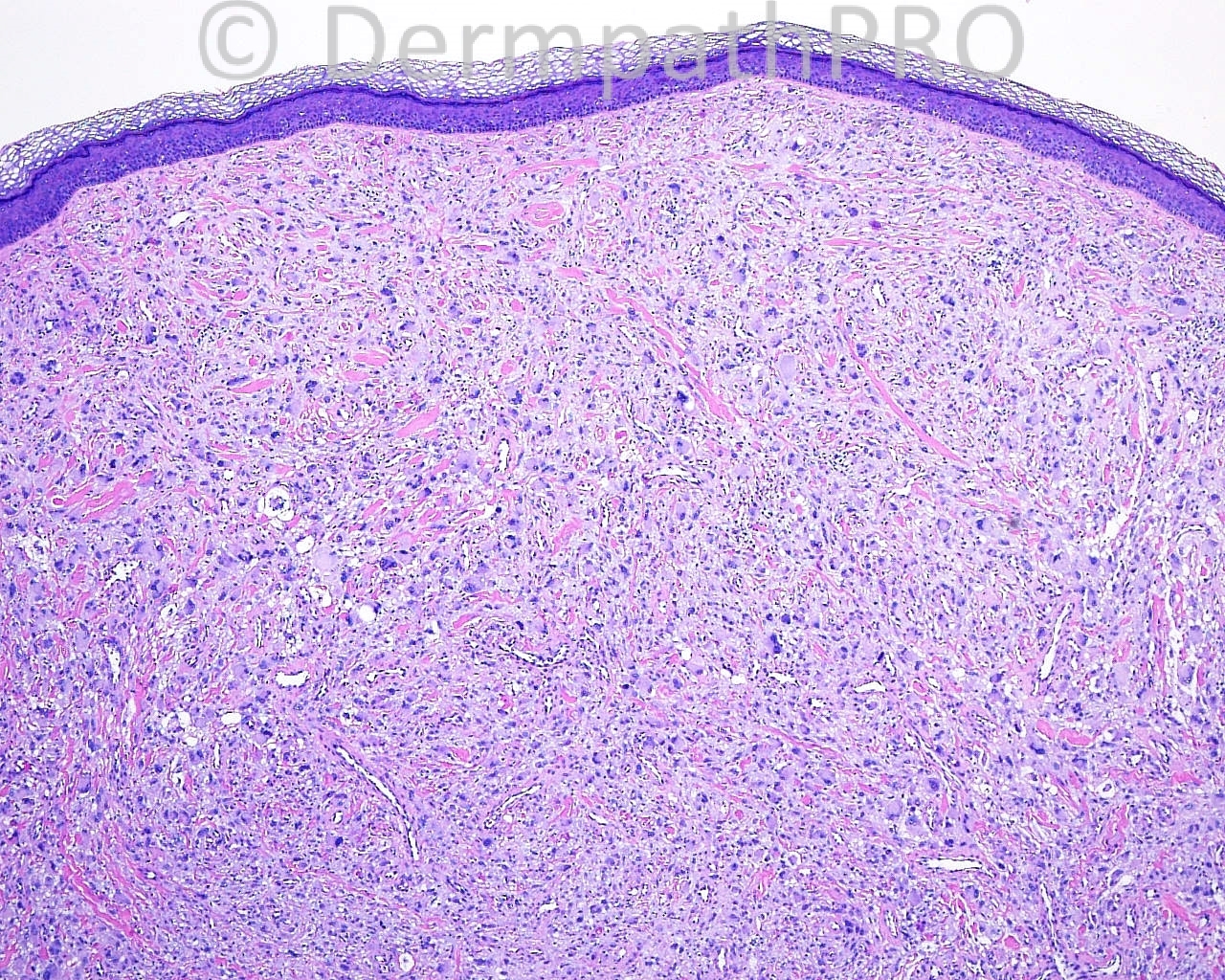
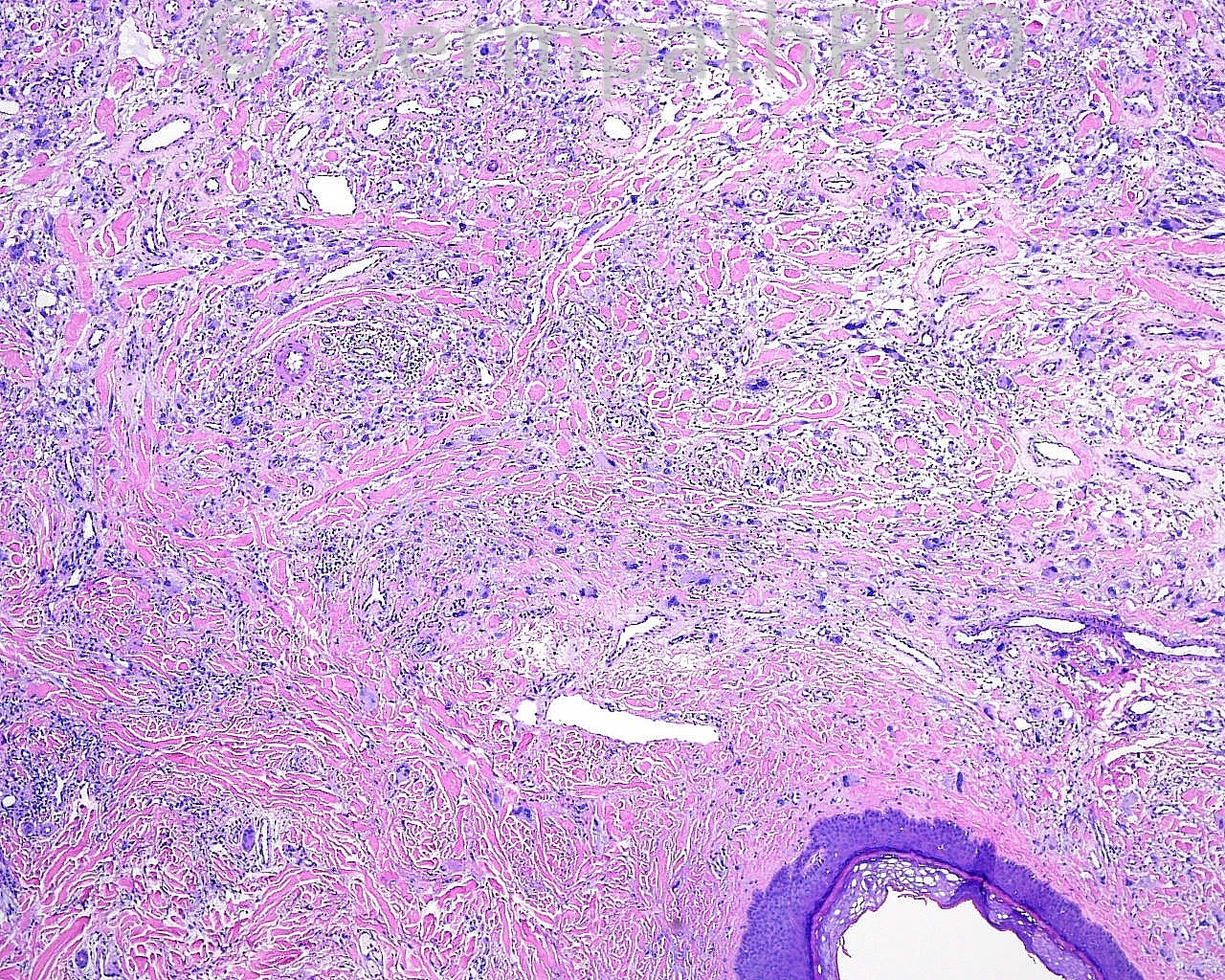
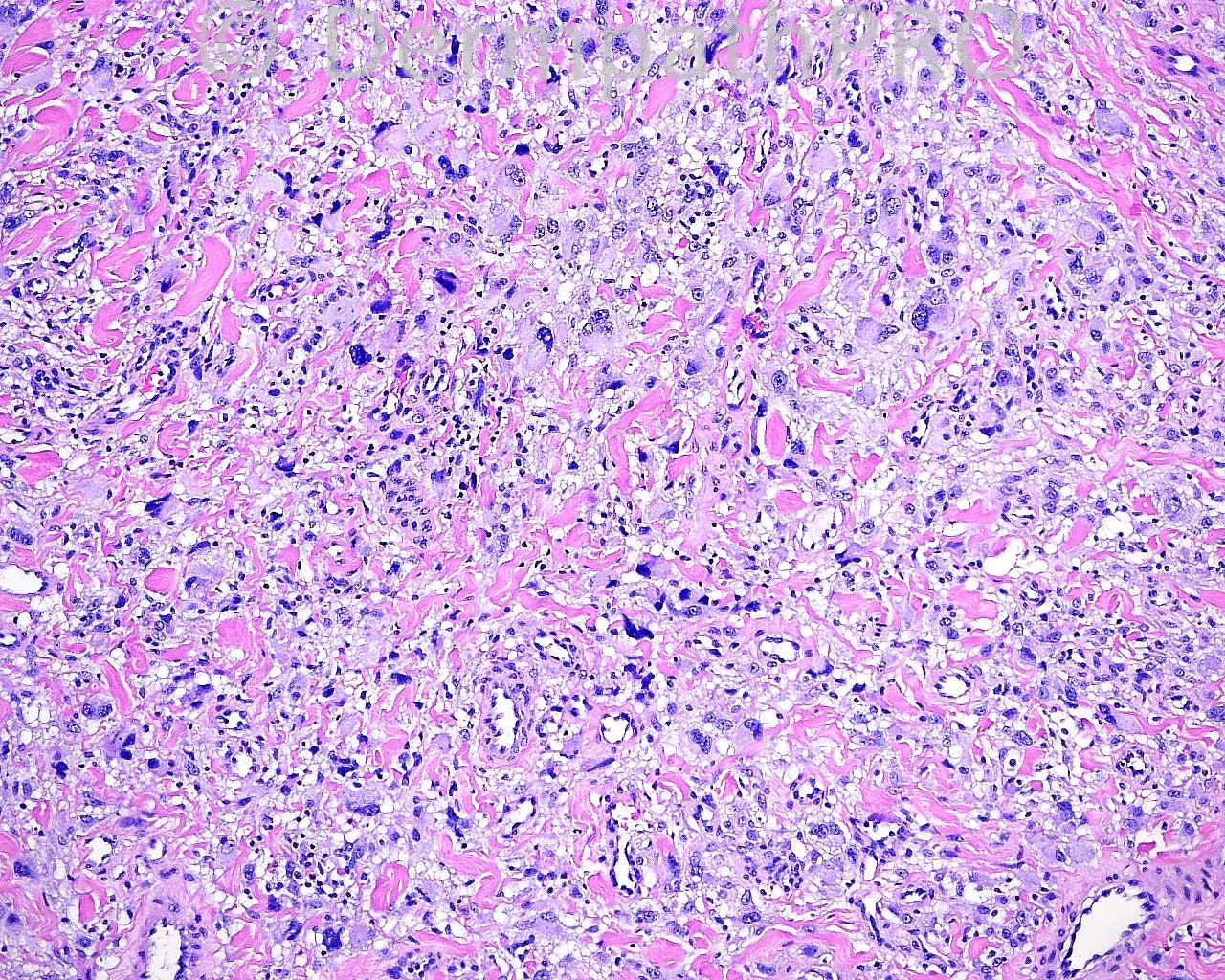
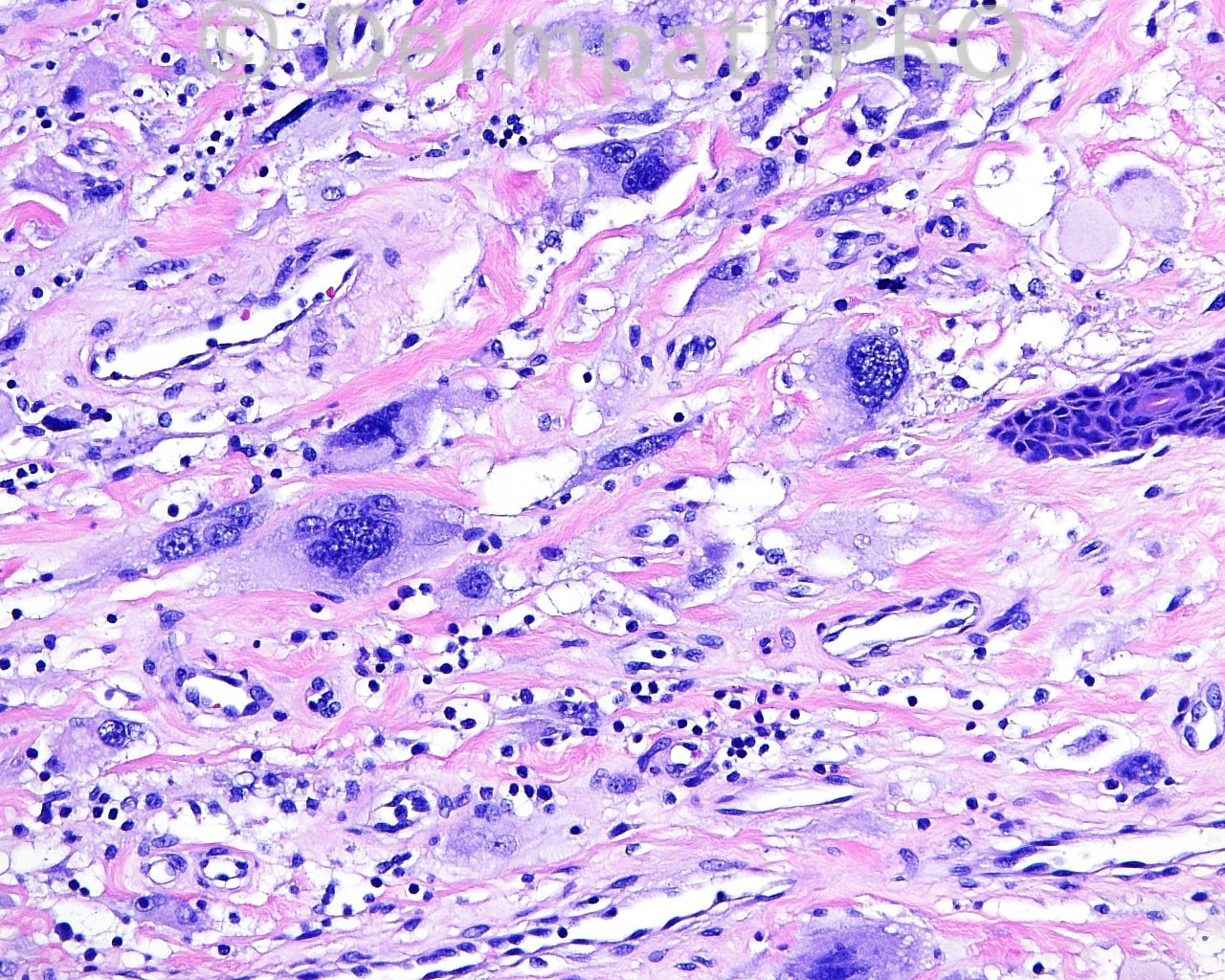
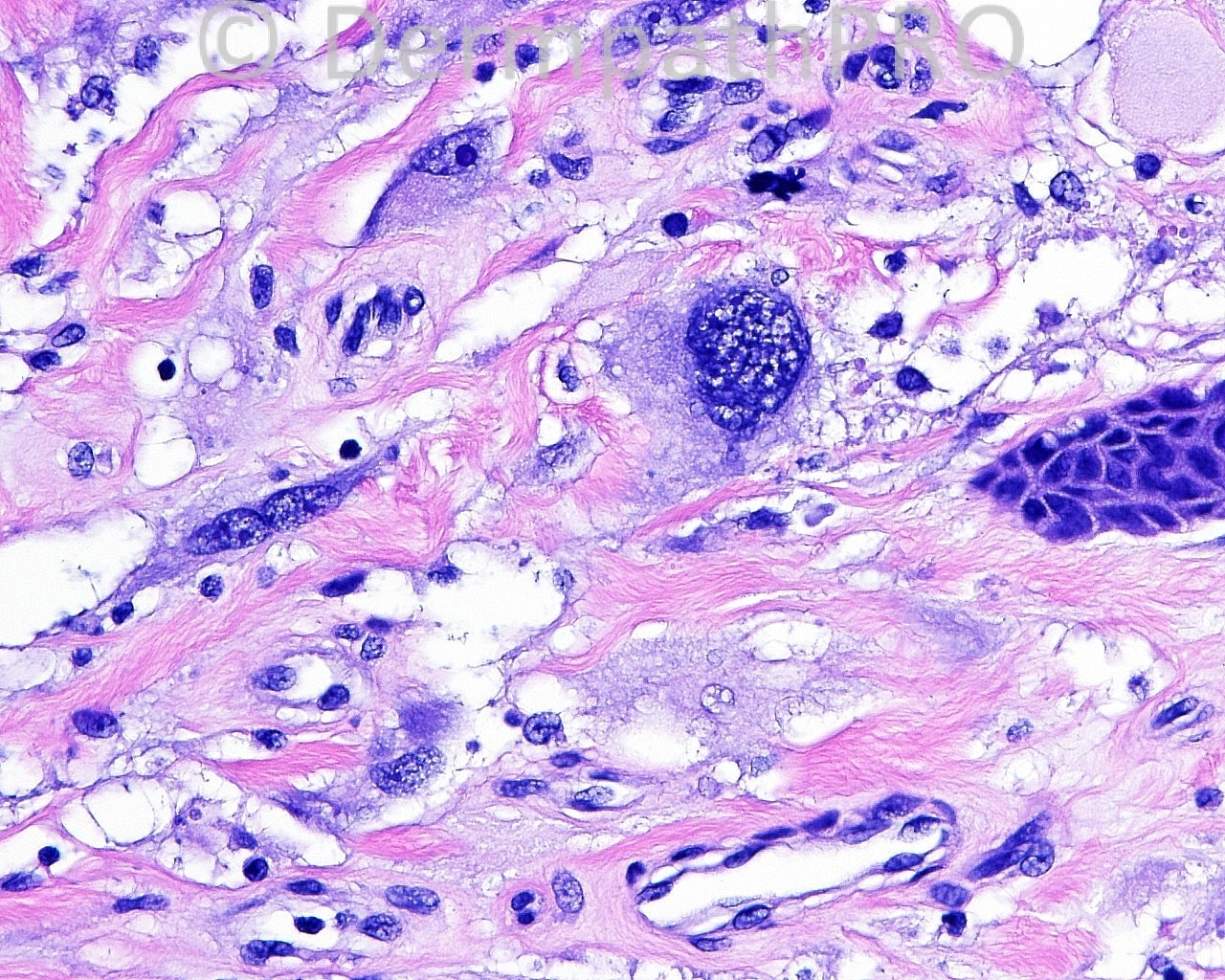
50 year old female with a shave biopsy from right upper thigh.
User Feedback