Diagnostic Pearls : CT0114
30 year old female with right ankle, foot and heel ulcer, s/p recent traumatic injury. This is an excisional biopsy of the right ankle lesion.
Posted No value





BAD DermpathPRO Learning Hub: Diagnostic Clues


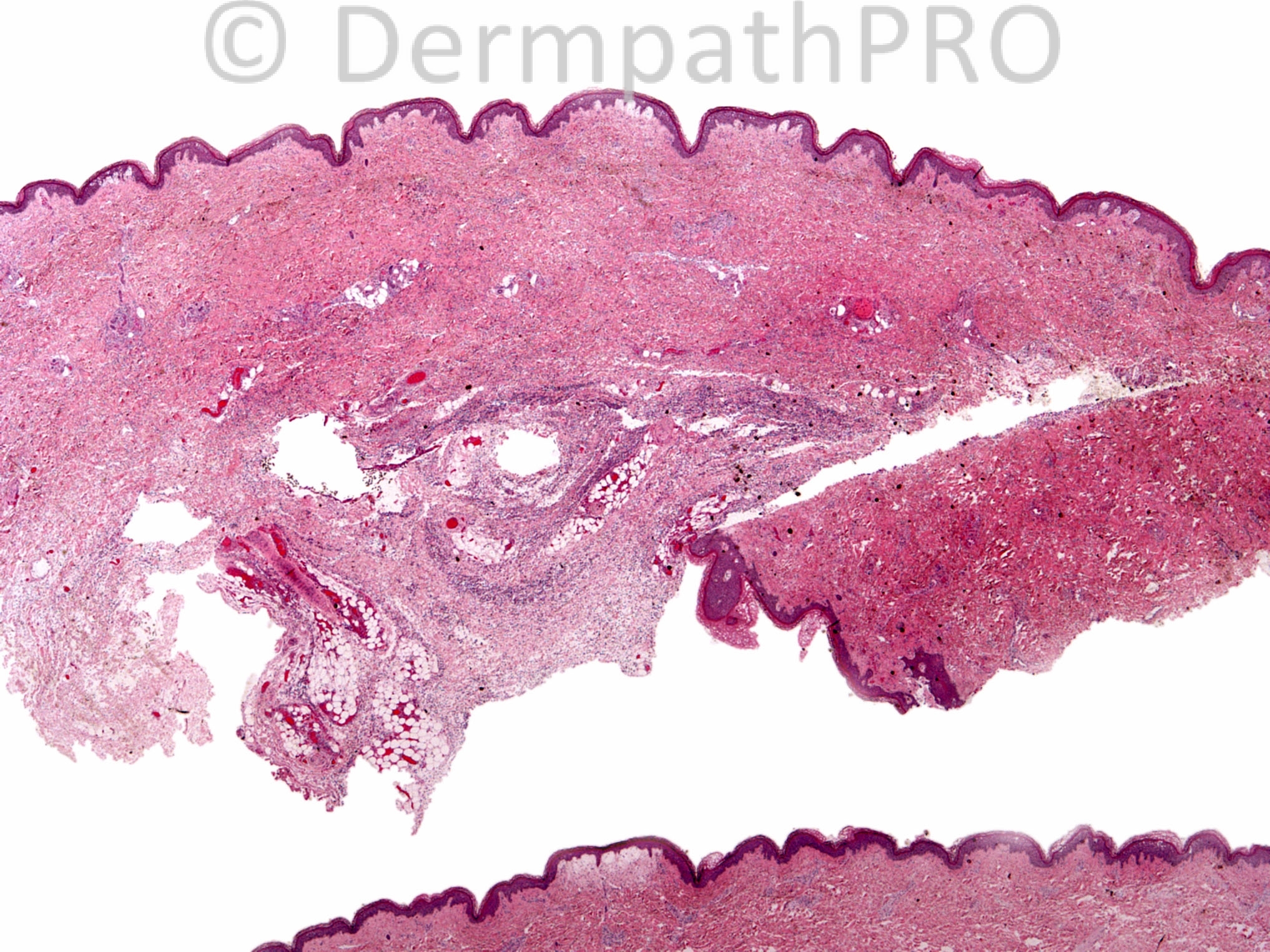
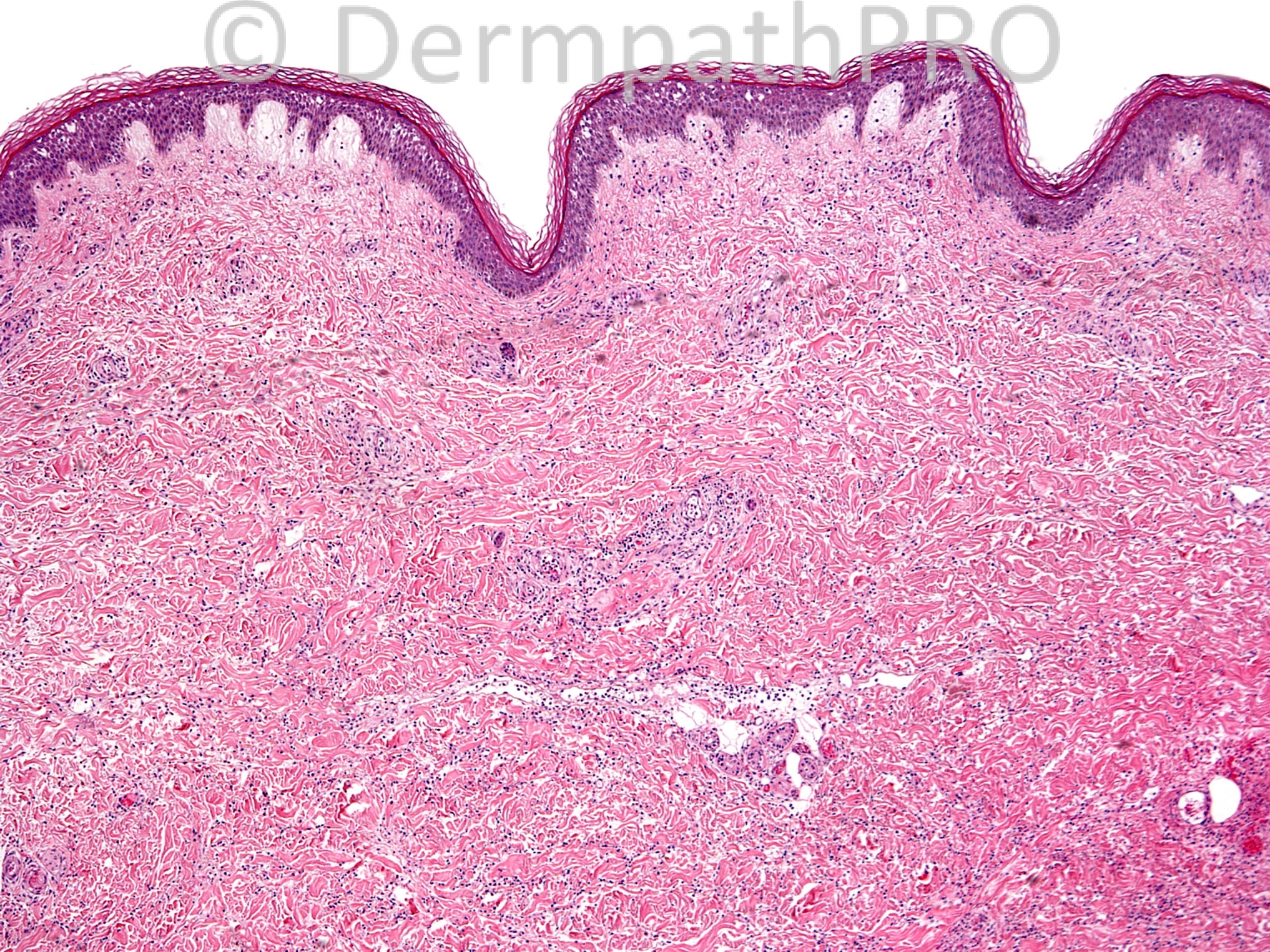
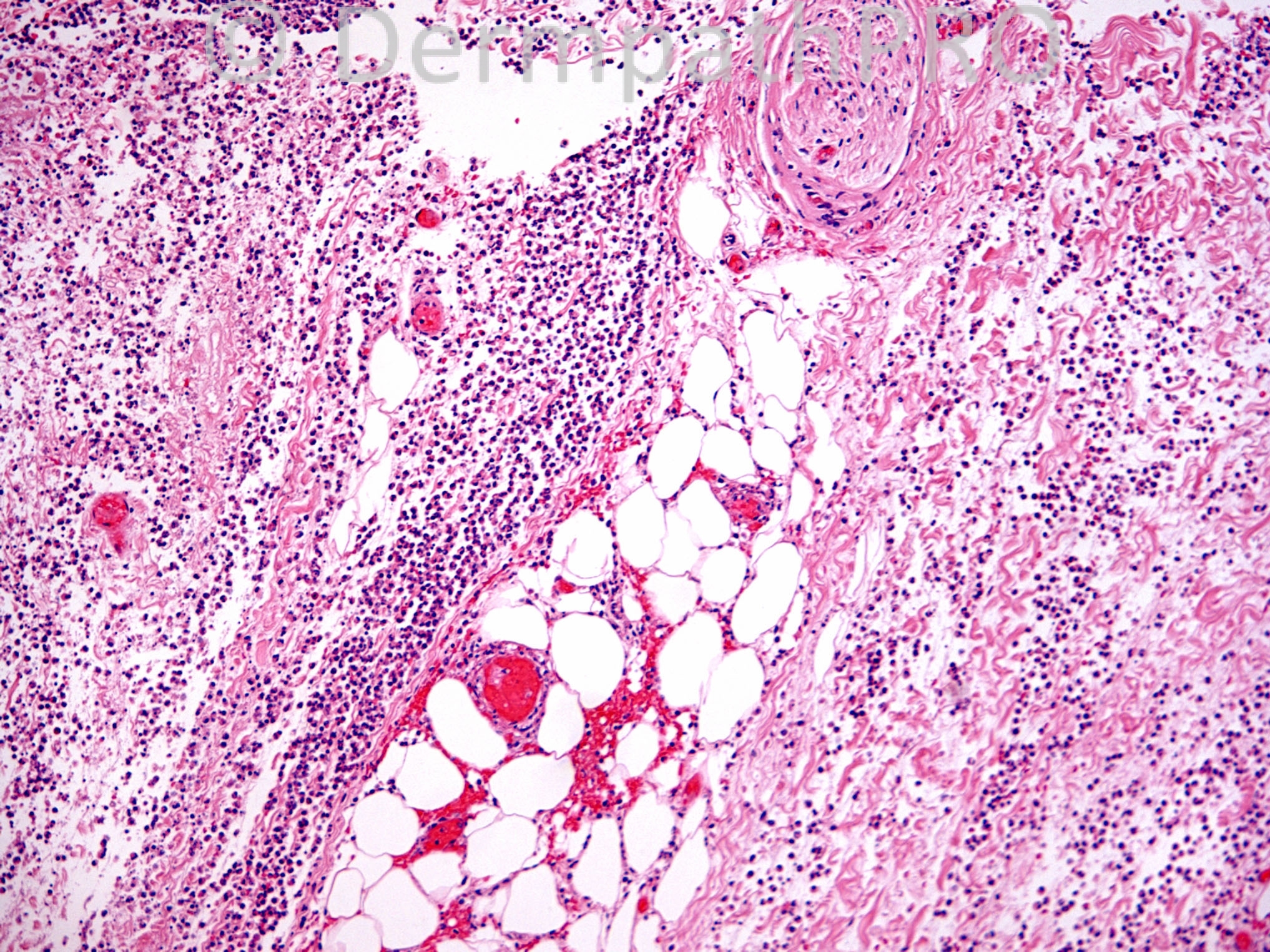

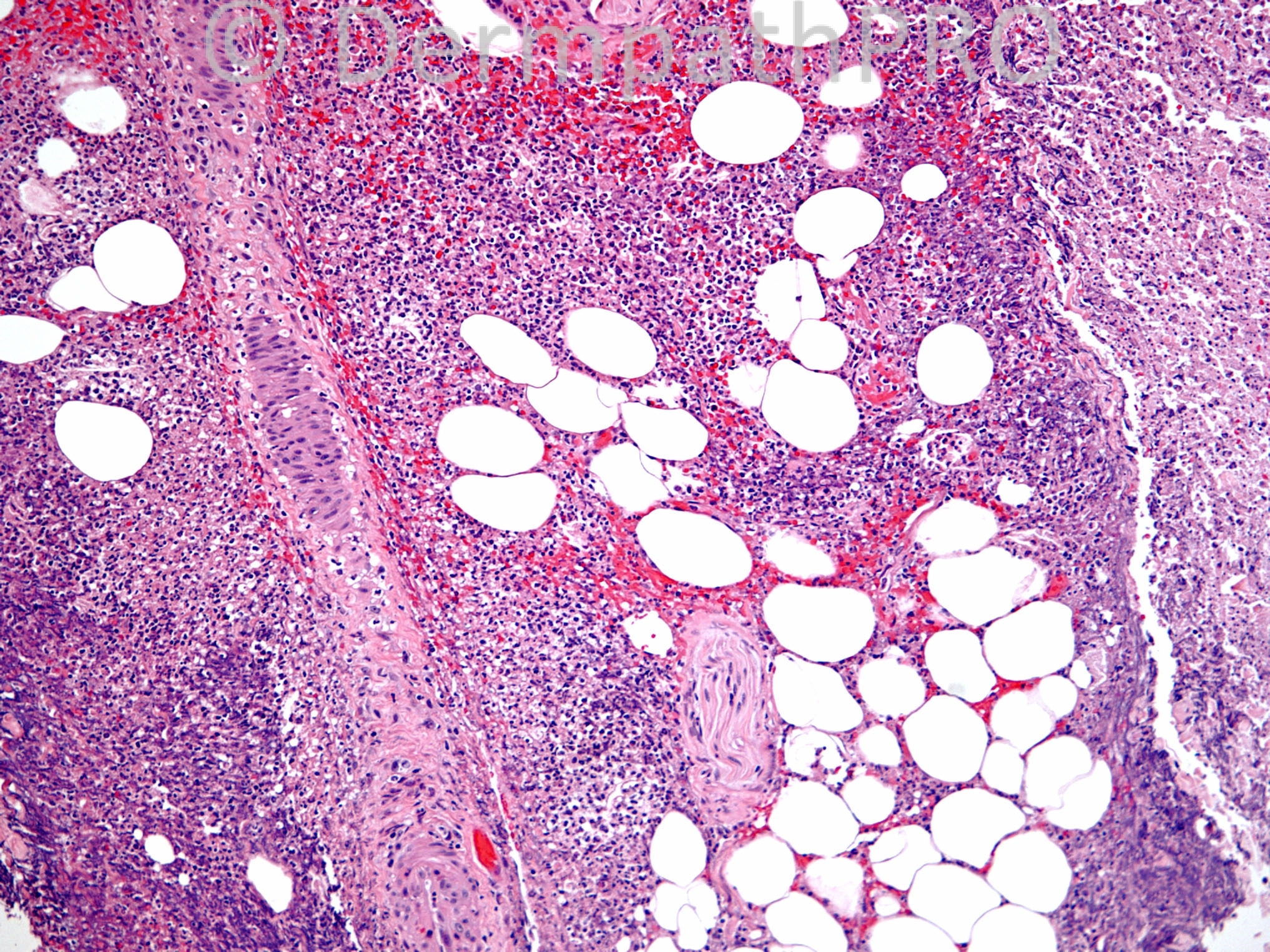
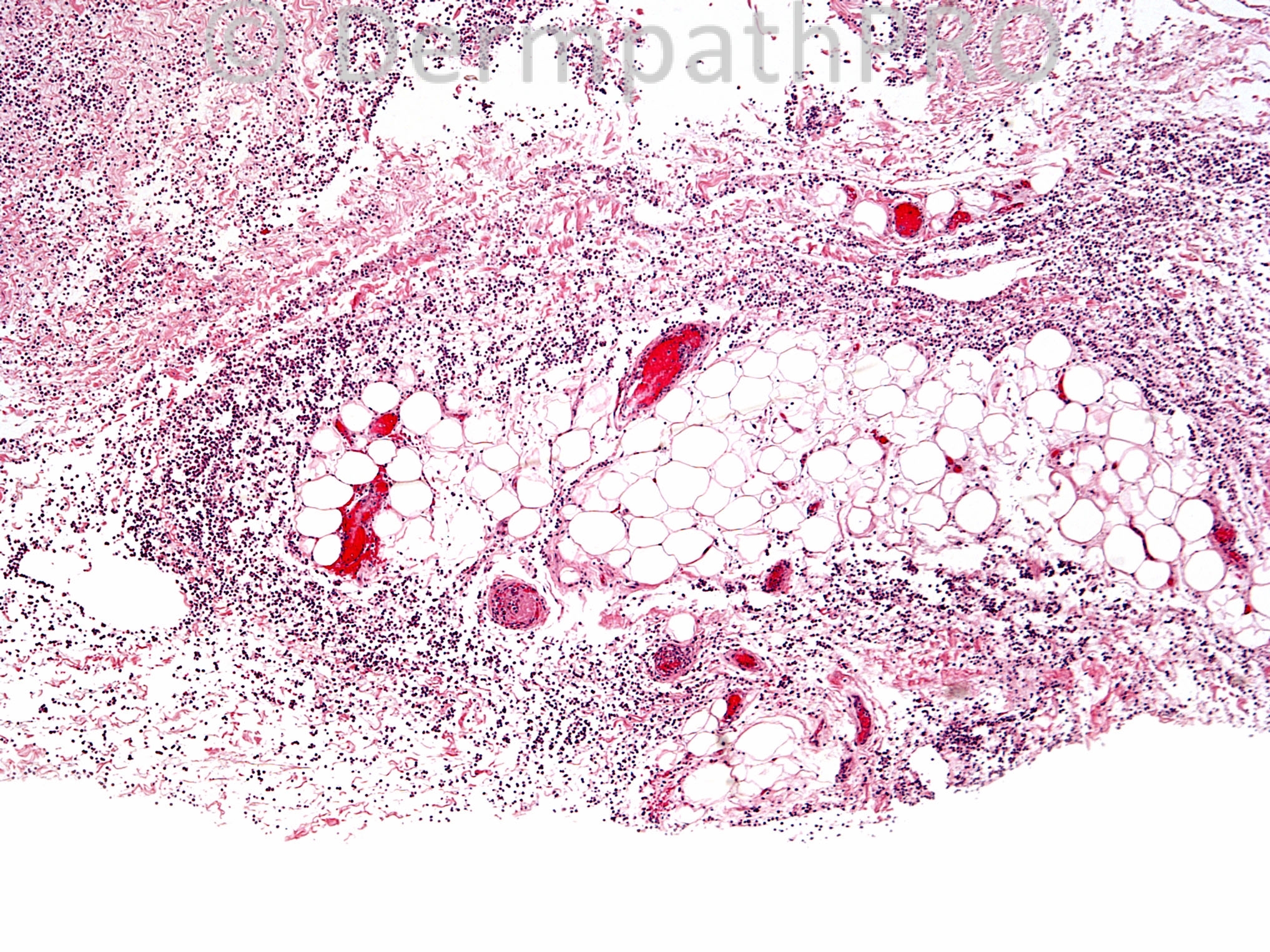
30 year old female with right ankle, foot and heel ulcer, s/p recent traumatic injury. This is an excisional biopsy of the right ankle lesion.
User Feedback