Please read the clinical history and view the images by clicking on them before you proffer your diagnosis.
Submitted Date :
(0 reviews)
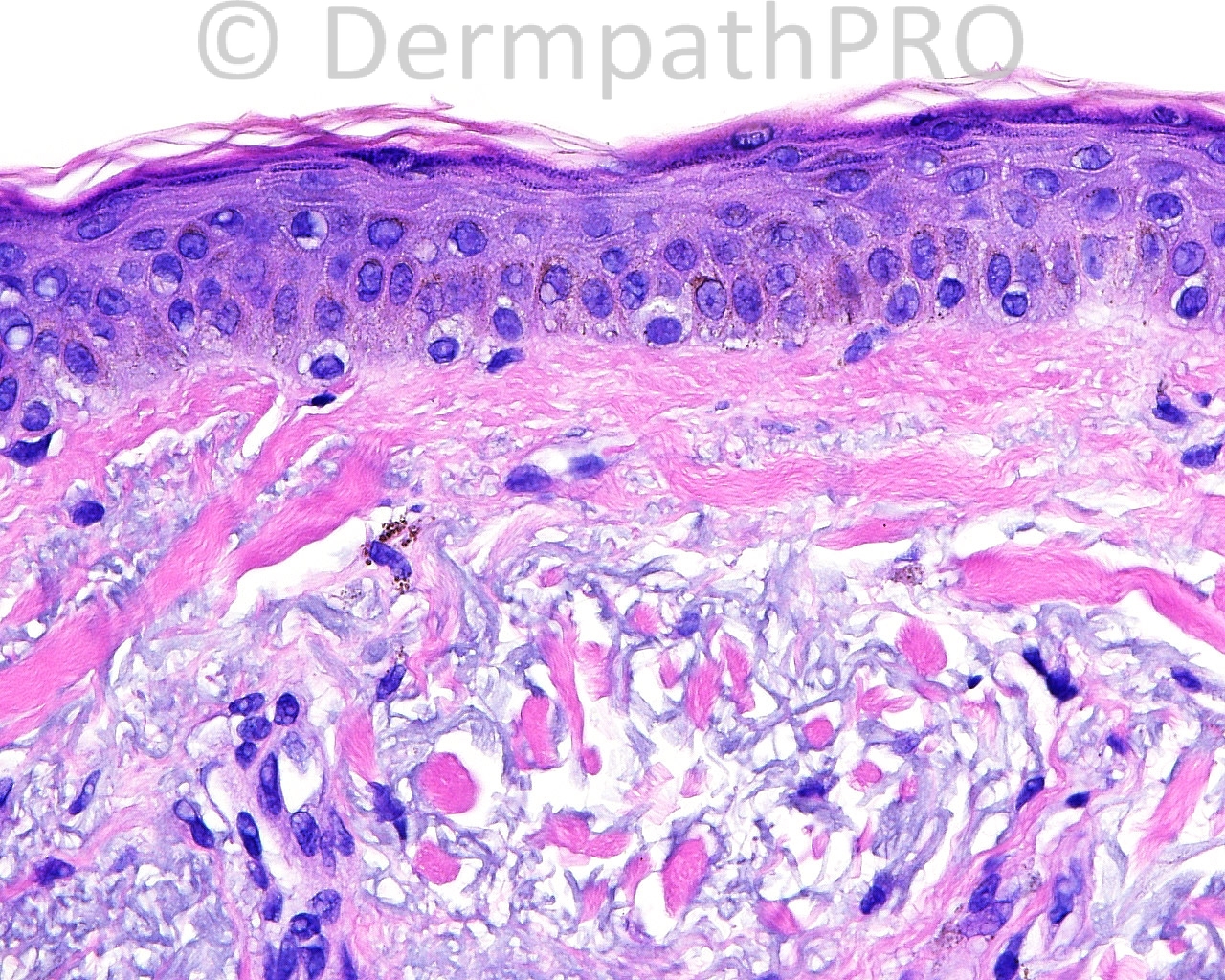
The patient is a 68-year-old woman who takes medication for ocular rosacea. A shave biopsy is taken of asymptomatic, blue-gray, macular pigment on the left cheek.







User Feedback