In this section we have spot diagnoses posted on a daily basis since June 2010, now over 4000! You can review the archived cases and read the suggested diagnoses by users and the final comment by the contributors. Case are uploaded each week day by 10 am UK time with the correct diagnosis will generally be posted at 8 pm UK time. Why not view the most recent spot diagnosis and proffer a diagnosis?
Please read the clinical history and view the images by clicking on them before you proffer your diagnosis.
Submitted Date :
(0 reviews)
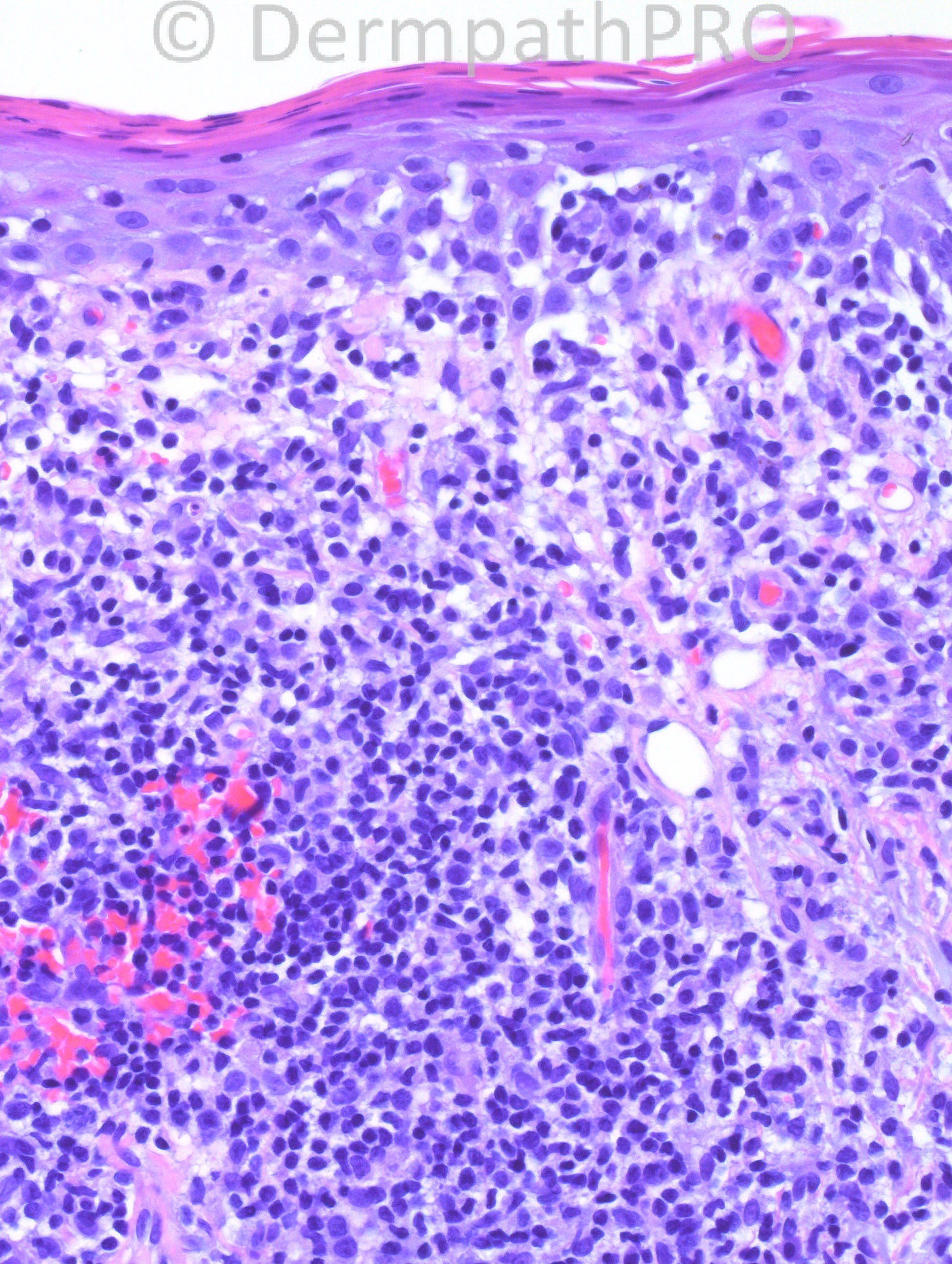
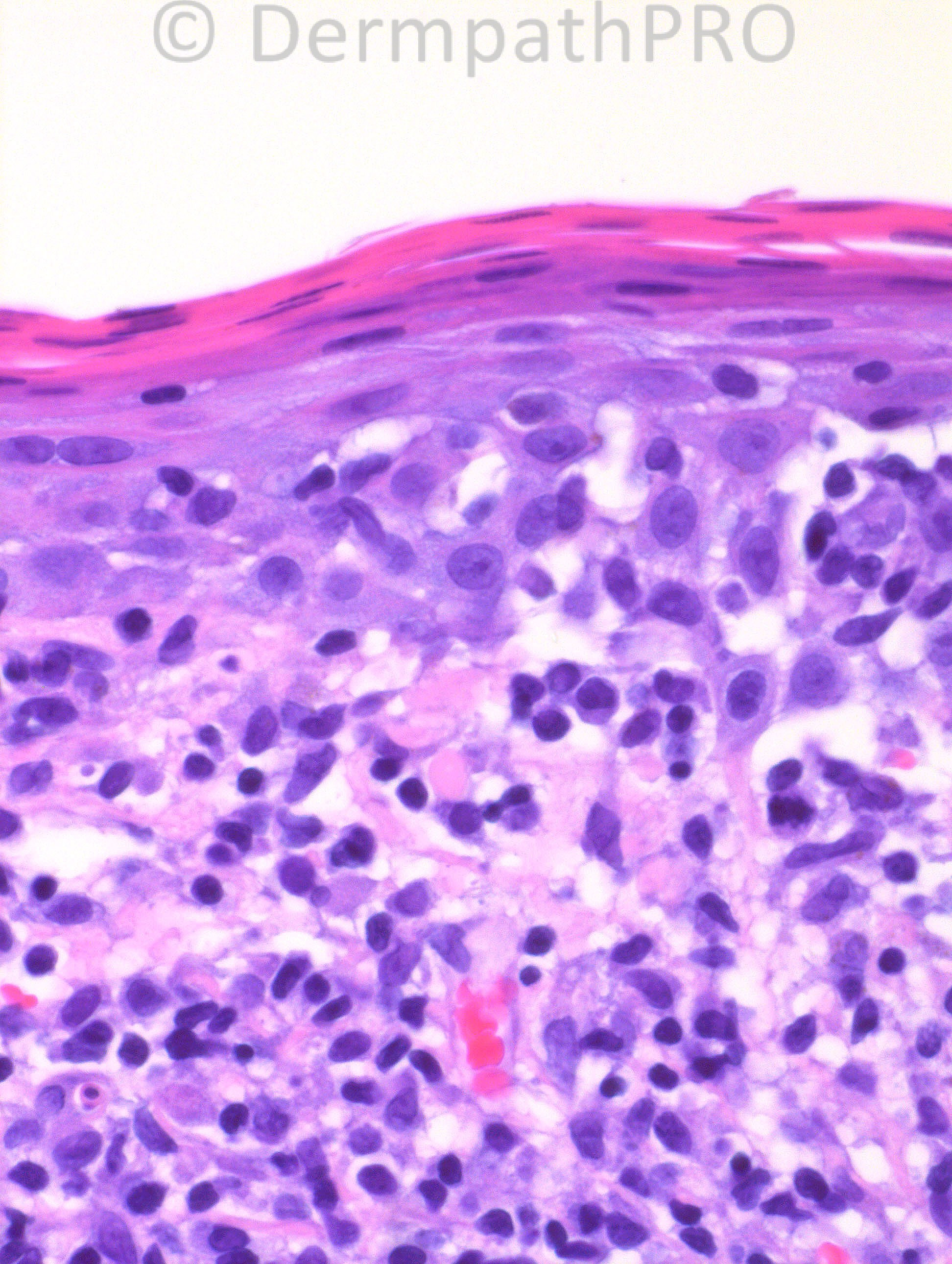
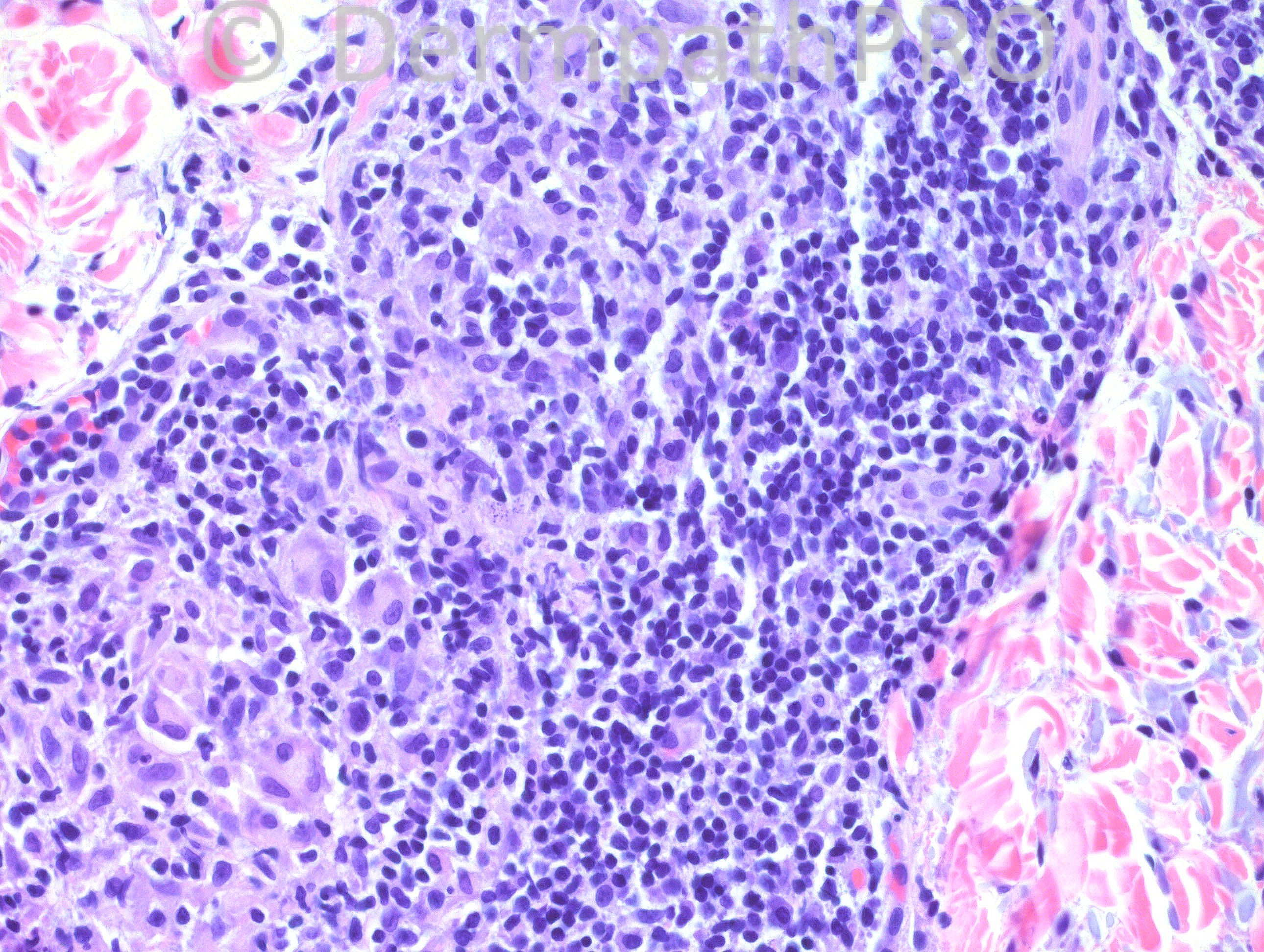
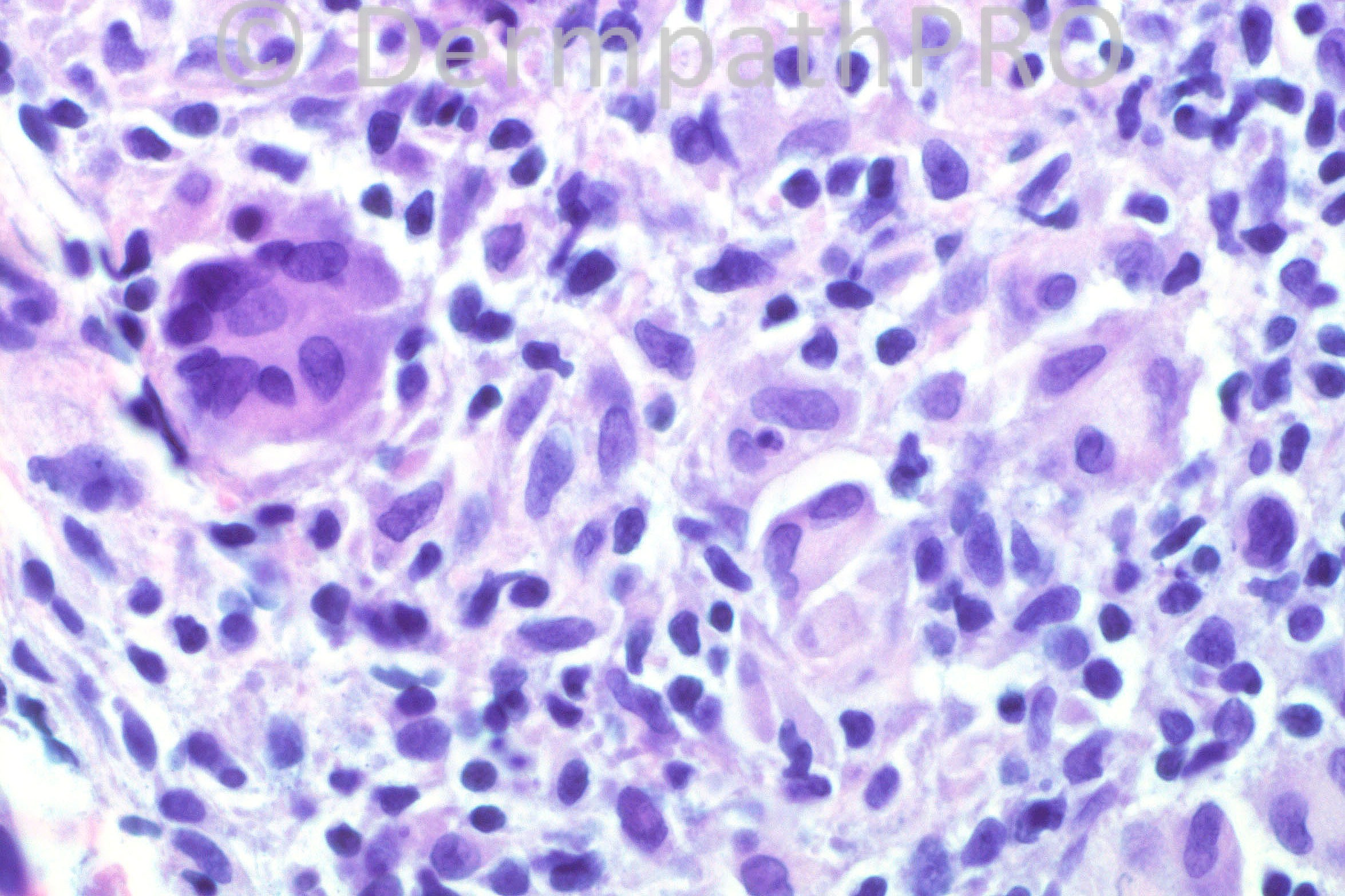
73-year-old male with a history of recurring granulomatous and necrotic lesions of uncertain etiology. A thigh biopsy from 2008 was read as “lichenoid and granulomatous dermatitis with eosinophils,†and other biopsies (from arm, trunk, and thigh) from 2009 as spongiotic dermatitis with eosinophils. On 1/11/2013, two biopsies were performed: one from the back, which was a “mature†lesion, and another from the right arm, which was a “new†lesion. The one that is shown here is the new lesion from the arm. The “mature†lesion showed ulceration, and had a more dense lymphocytic and histiocytic proliferation.
User Feedback