Diagnostic Pearls : Case 2812- 16 April 2021
M75. h/o Ocular melanoma 2016. Developed nasal cavity mass.
Dr. Richard Carr
Posted 15/04/21
Posted 15/04/21
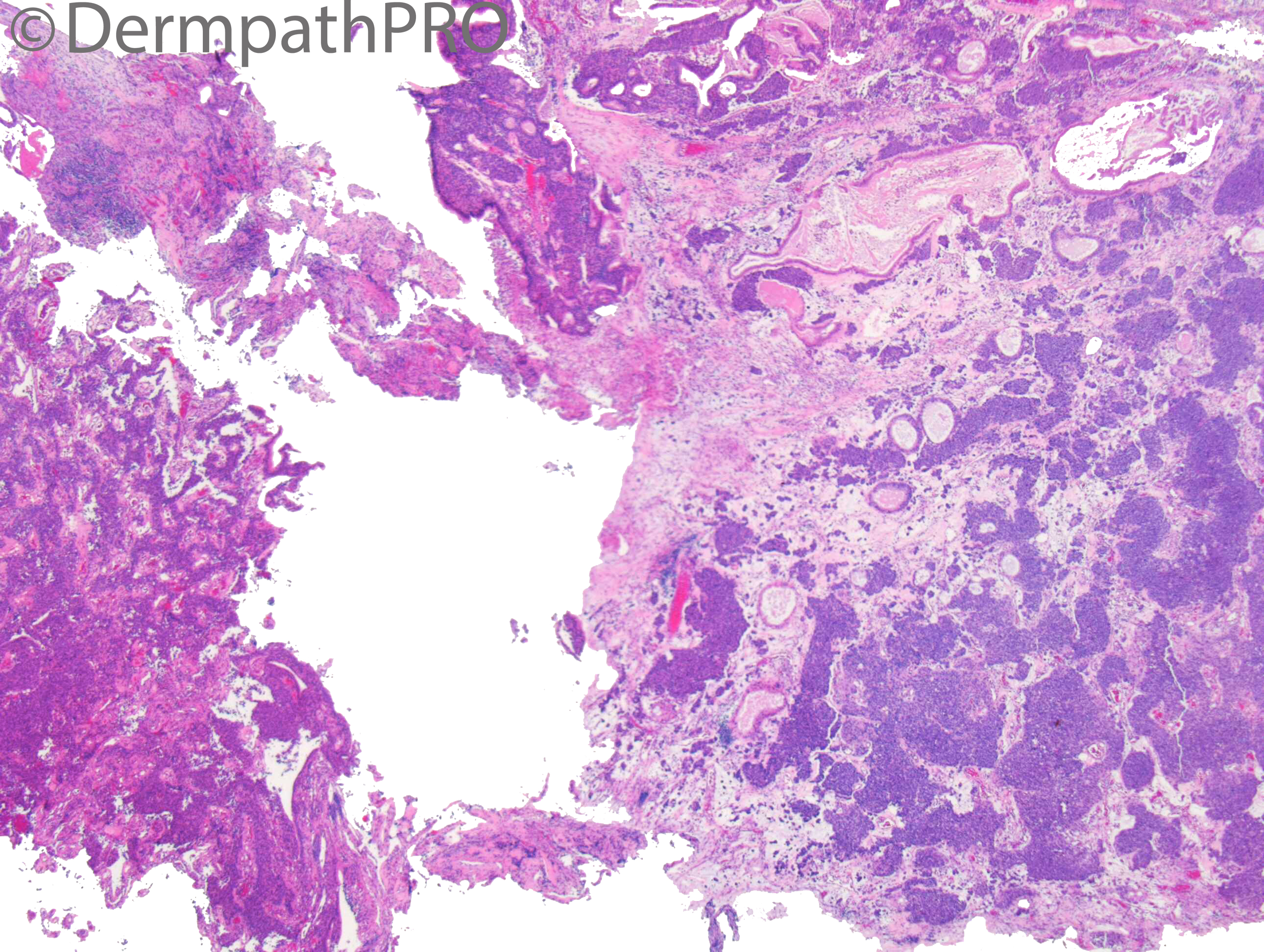
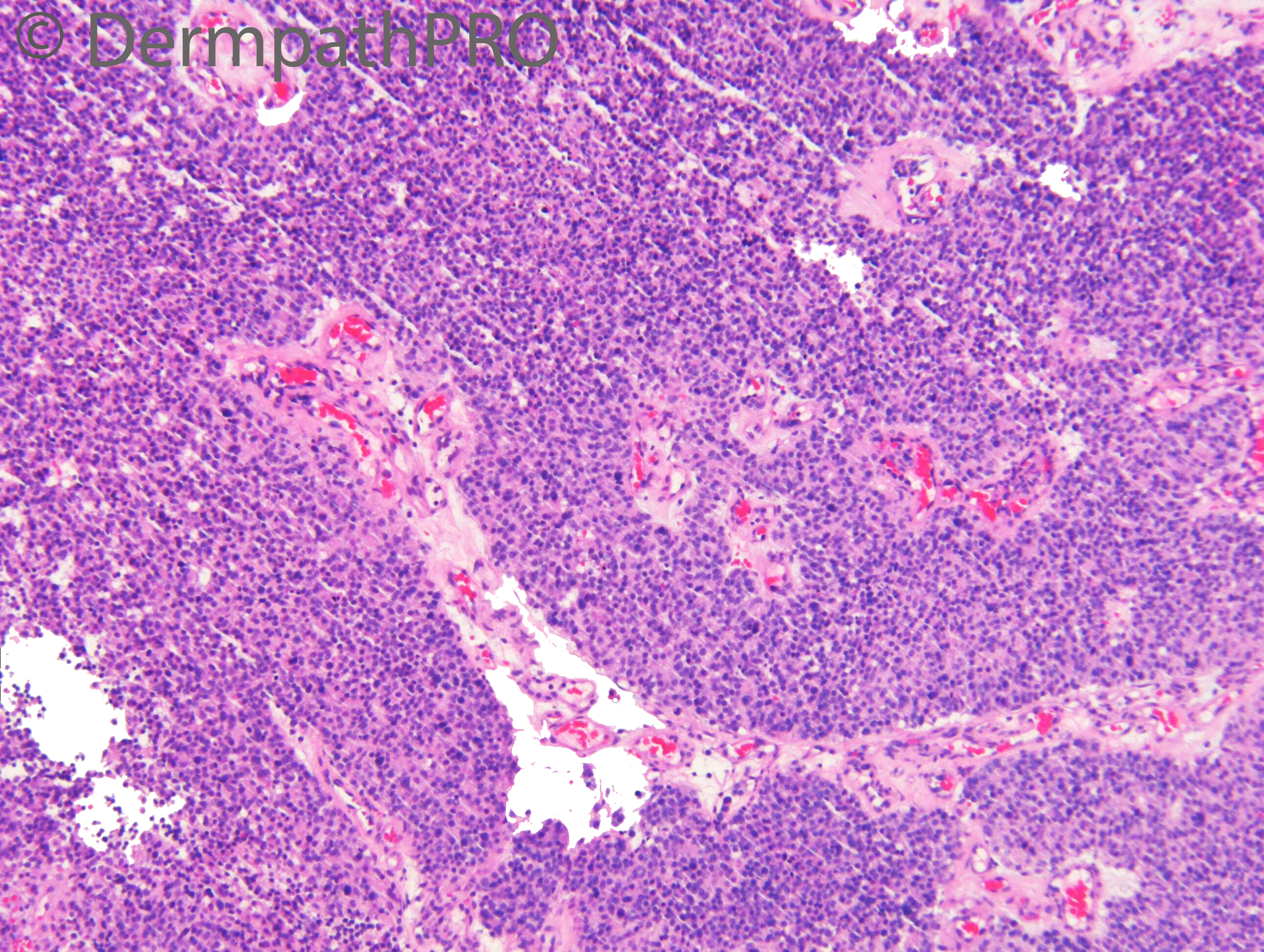
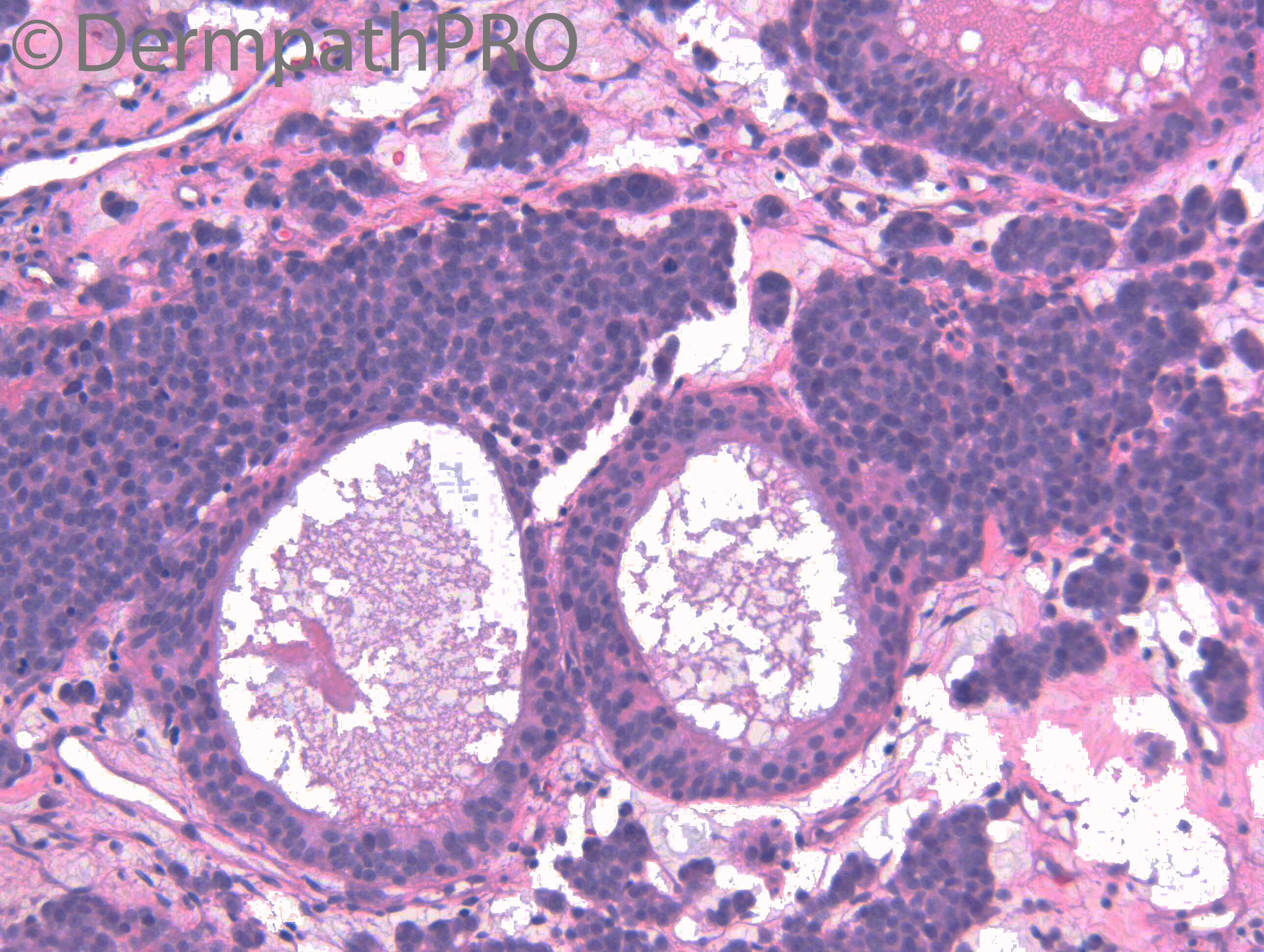
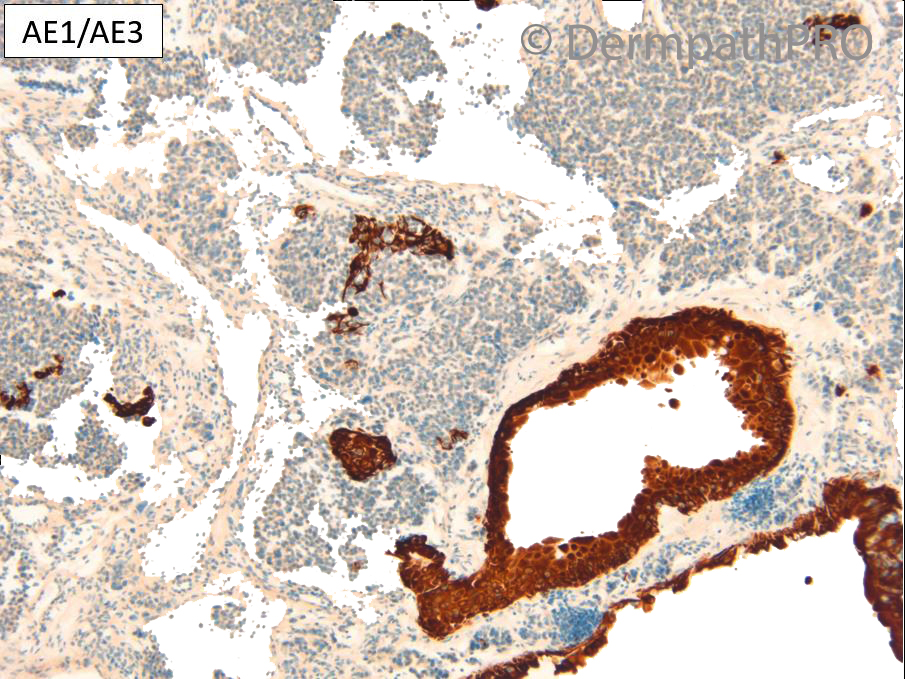
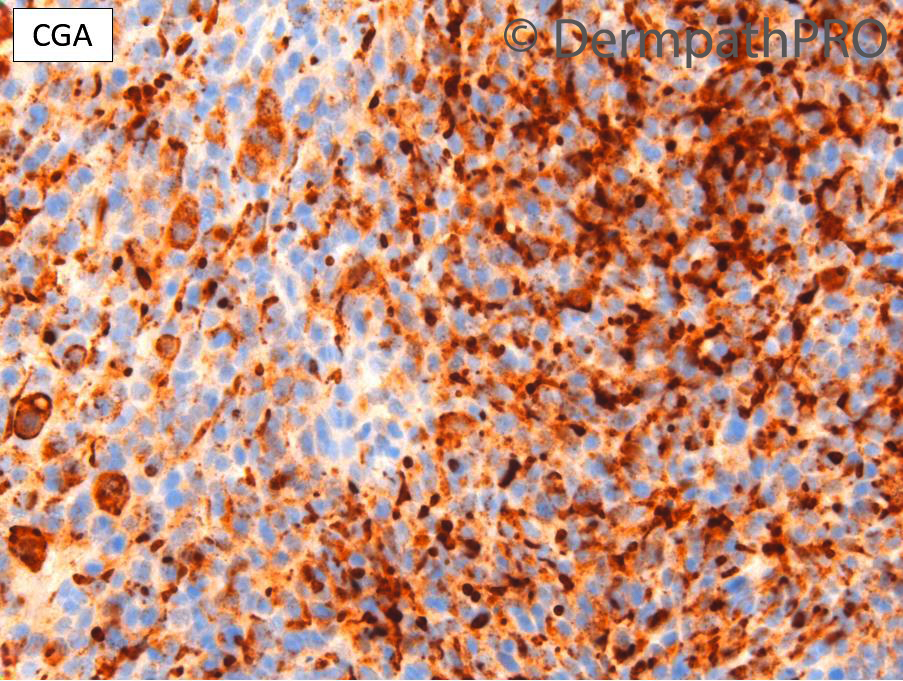
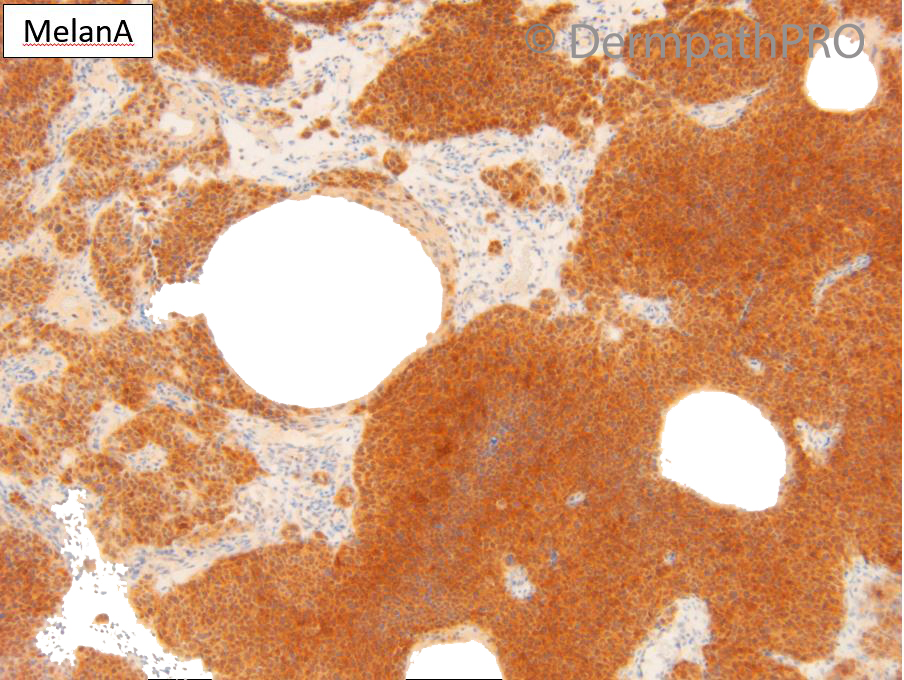
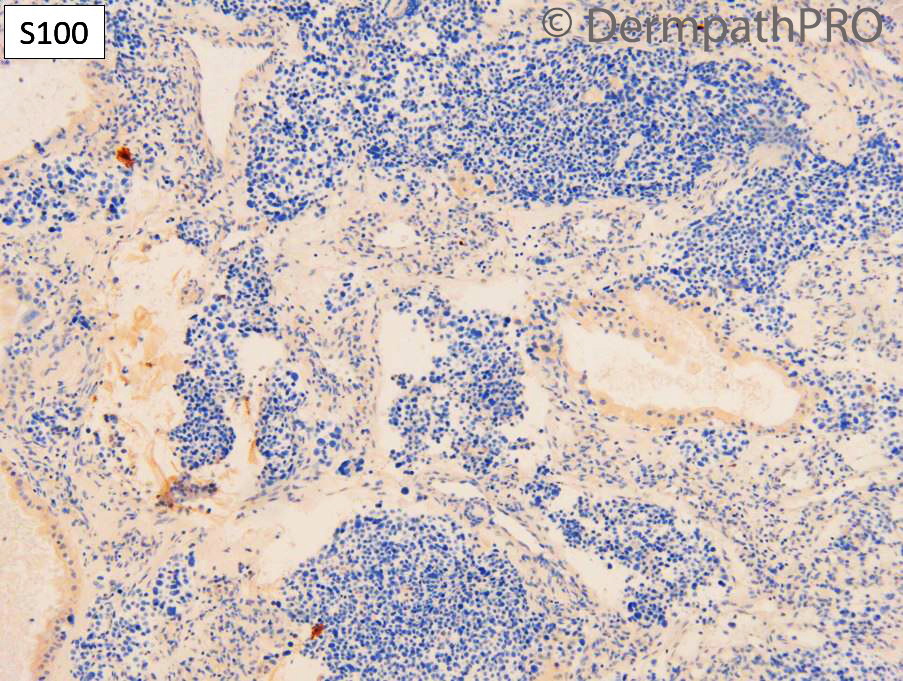
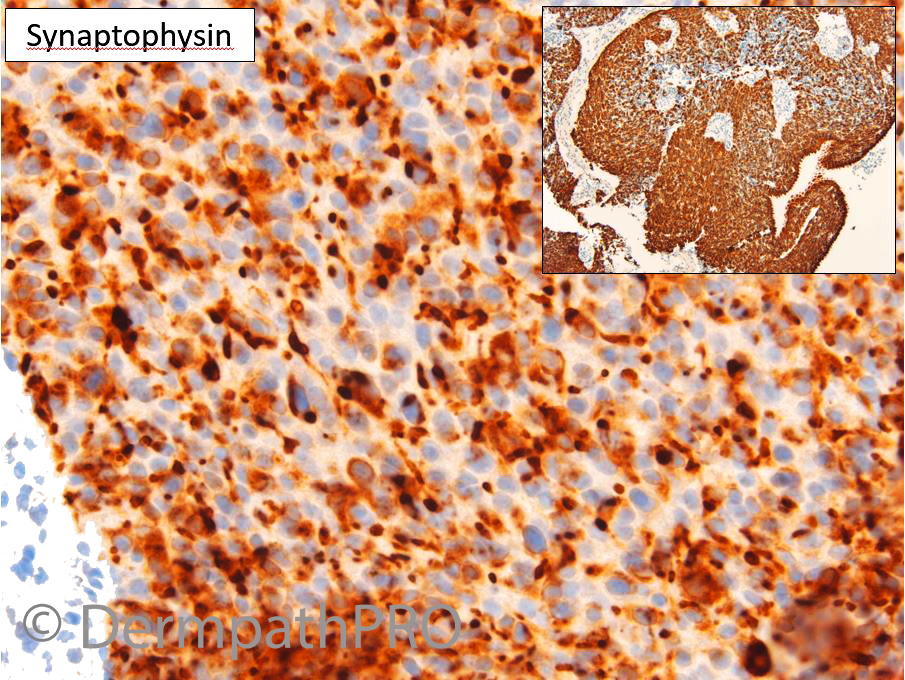
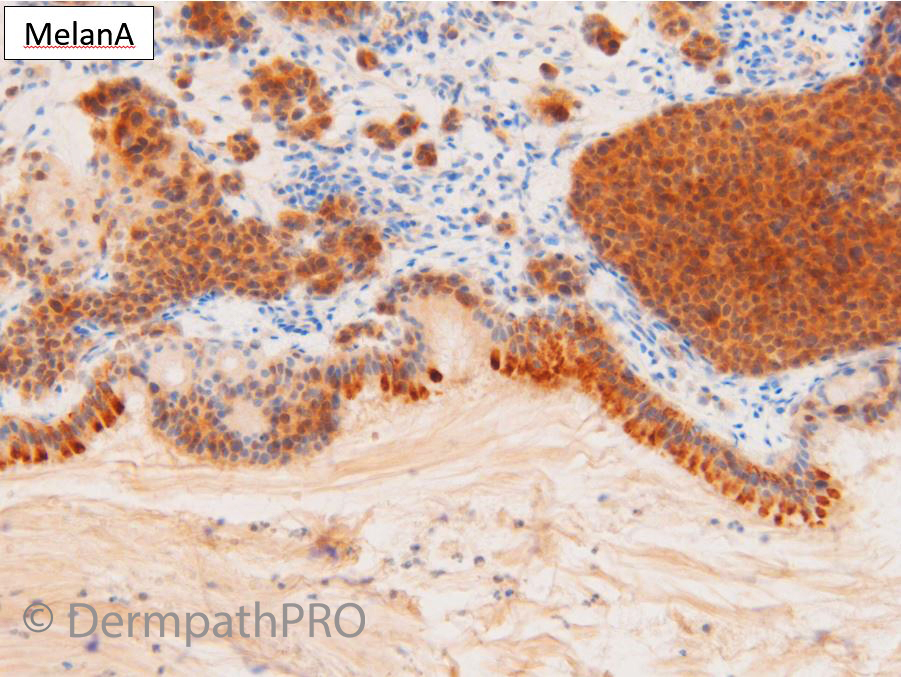
M75. h/o Ocular melanoma 2016. Developed nasal cavity mass.
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.