Diagnostic Pearls : Case 2996 - 30 December 2021
58F Punch biopsy right leg ?seborrhoeic keratosis ?BCC
Saleem Taibjee
Posted 29/12/21
Posted 29/12/21
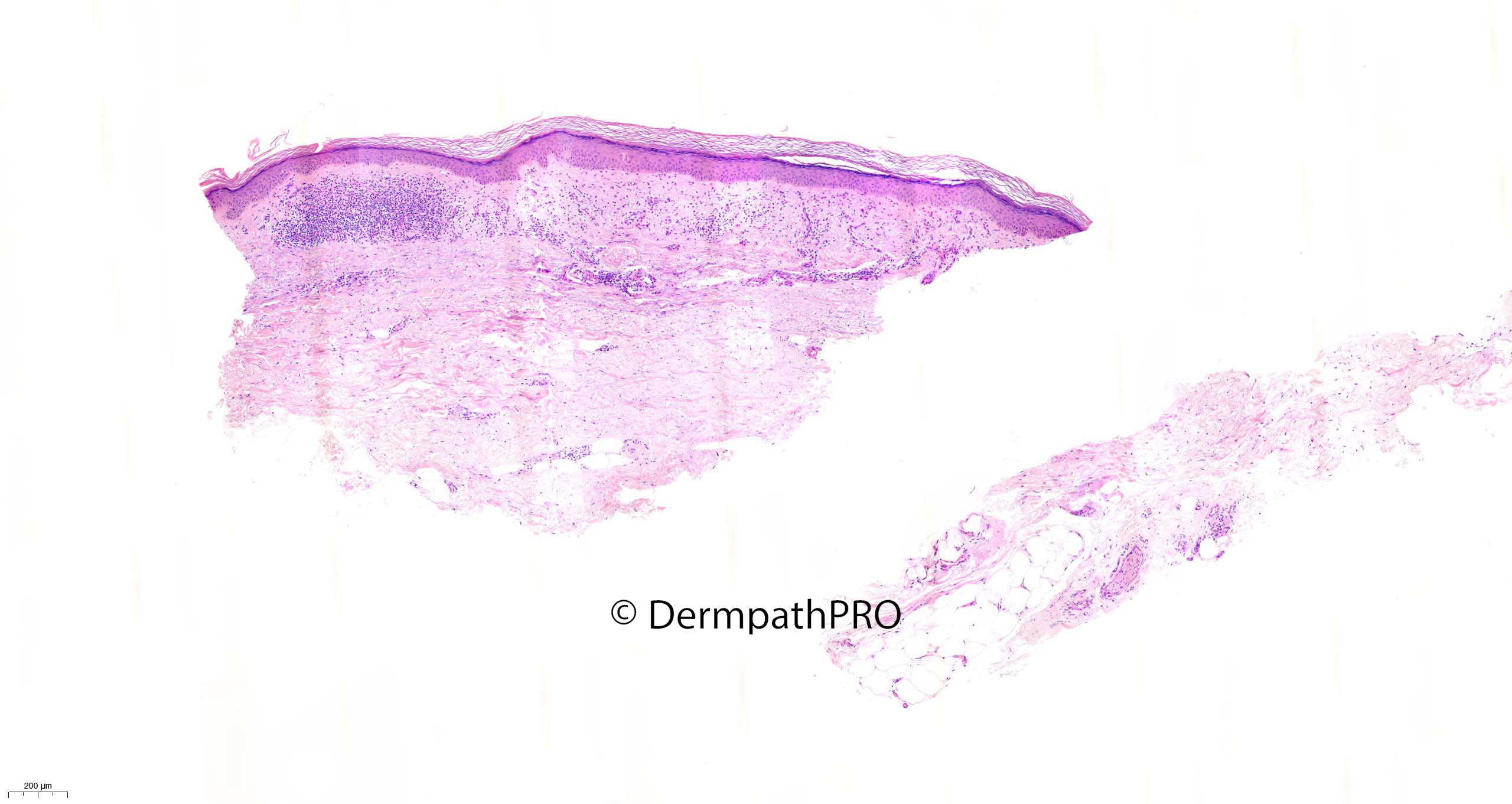
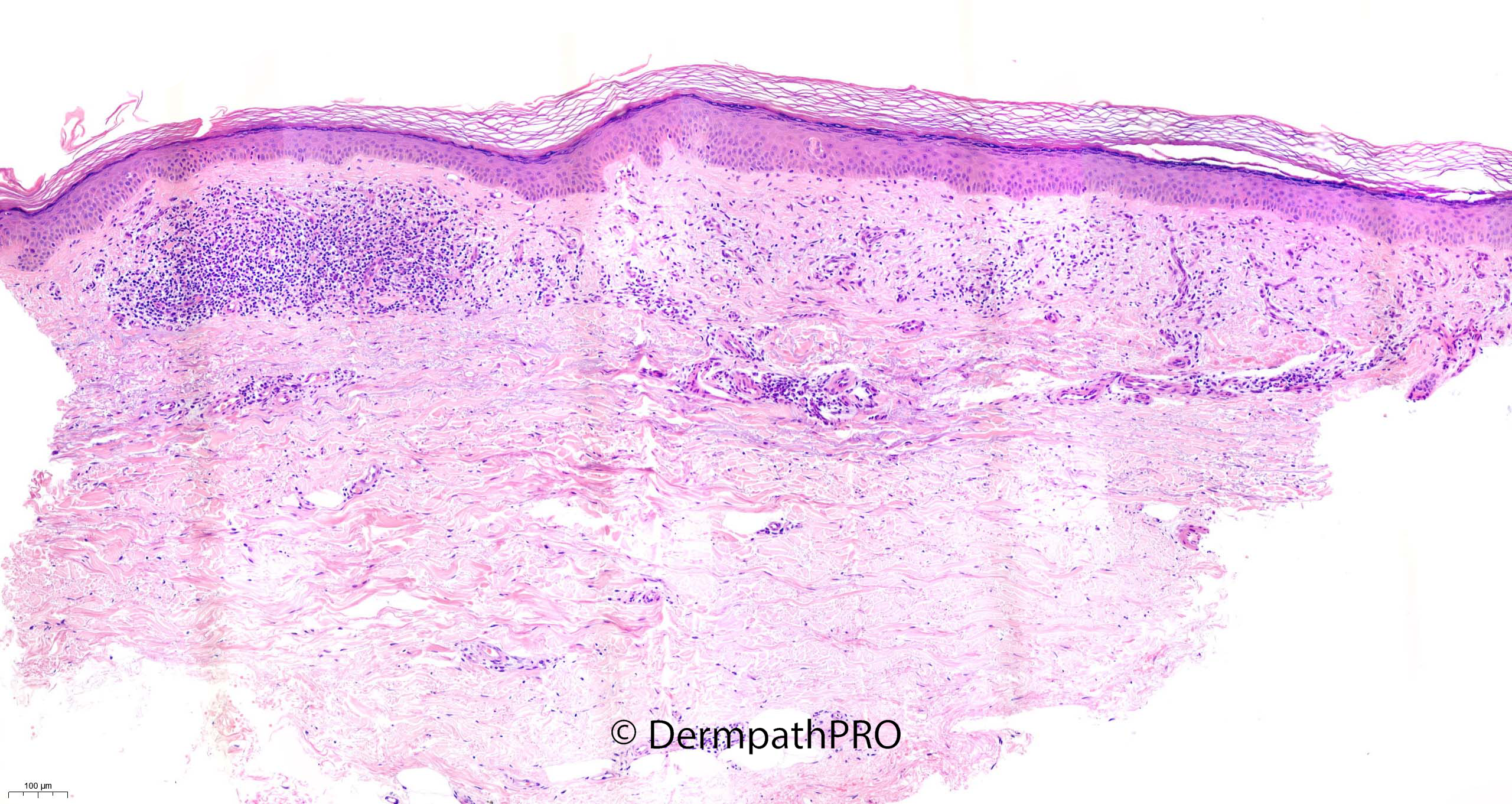
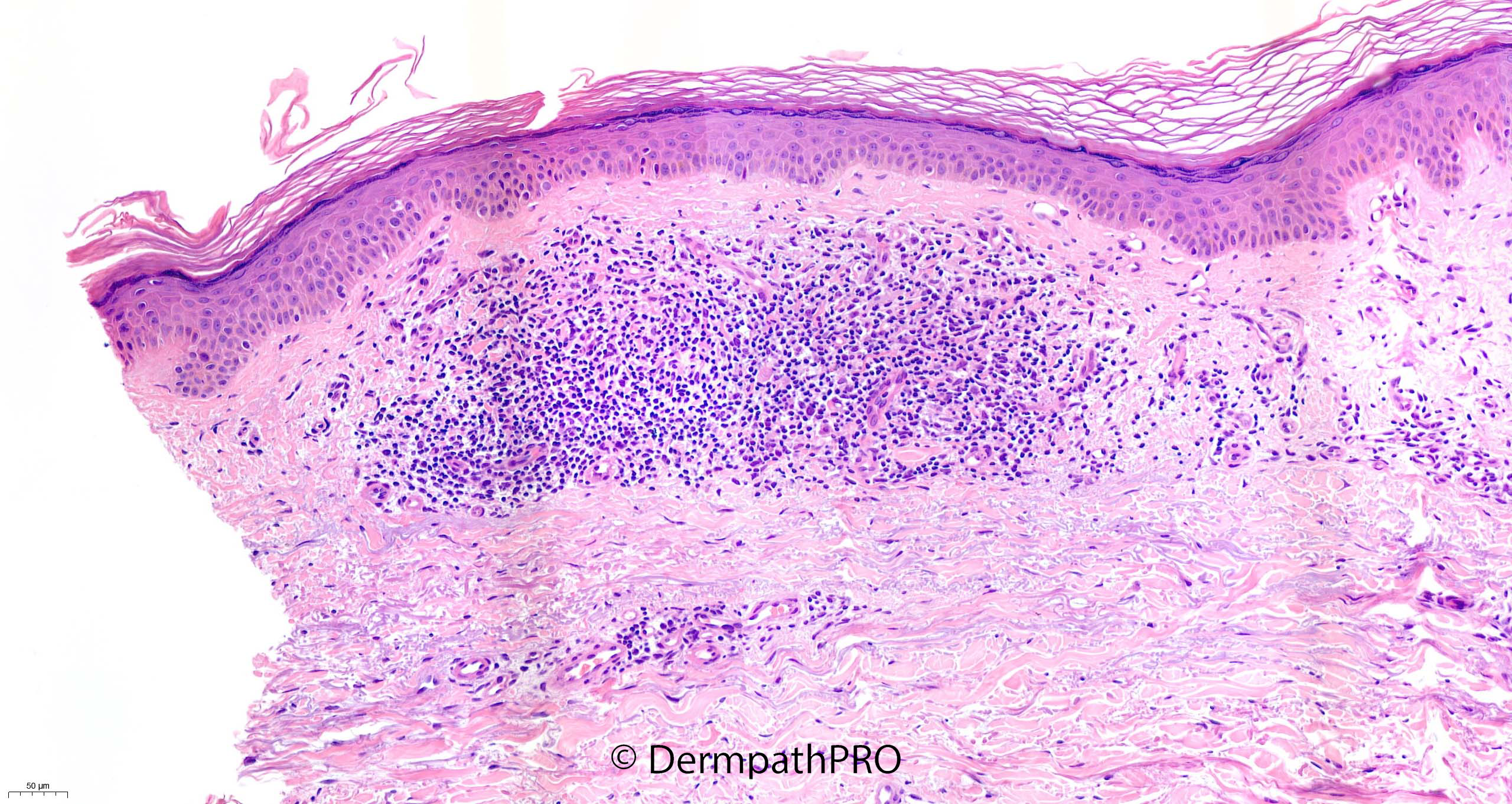
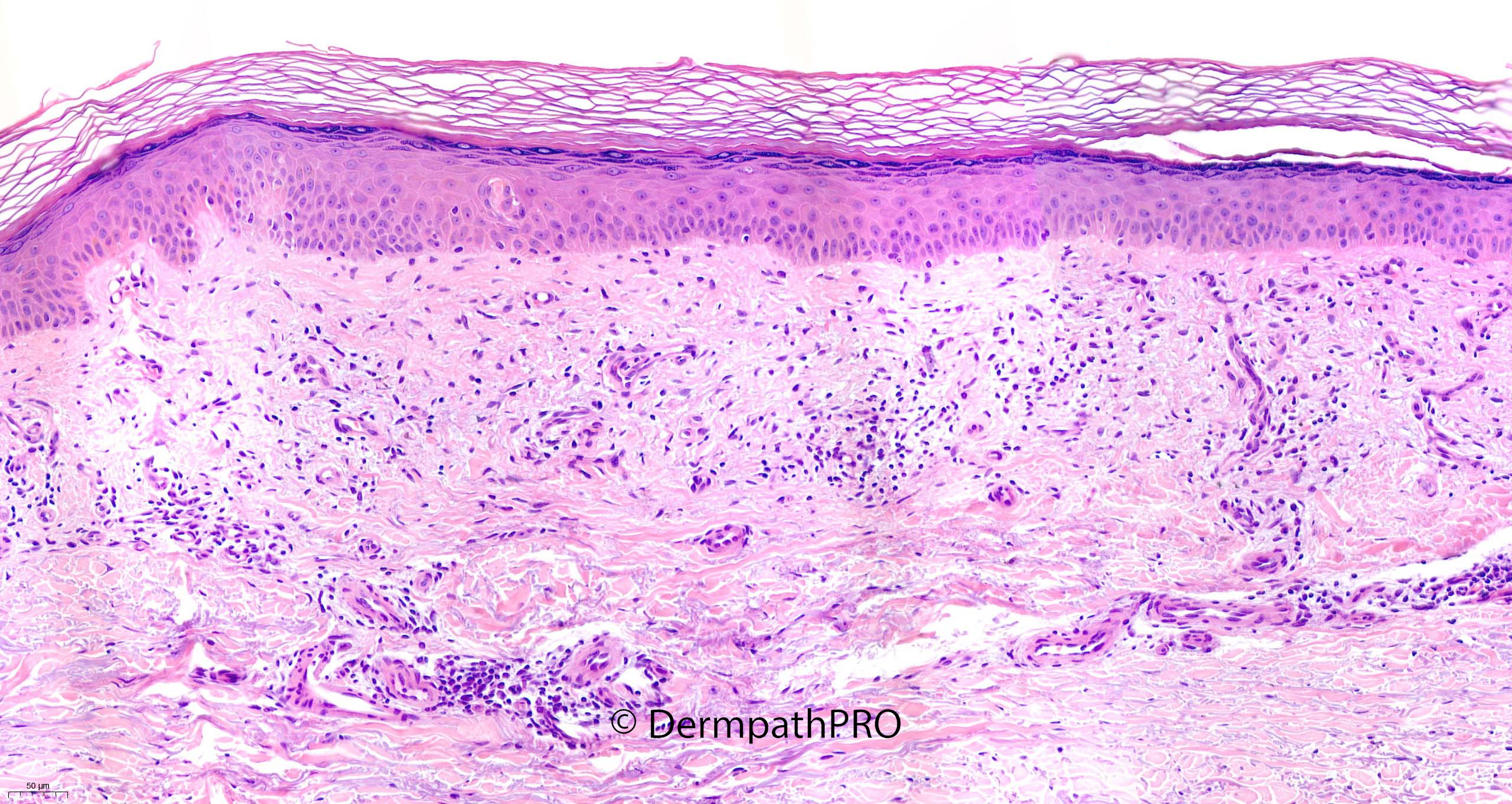
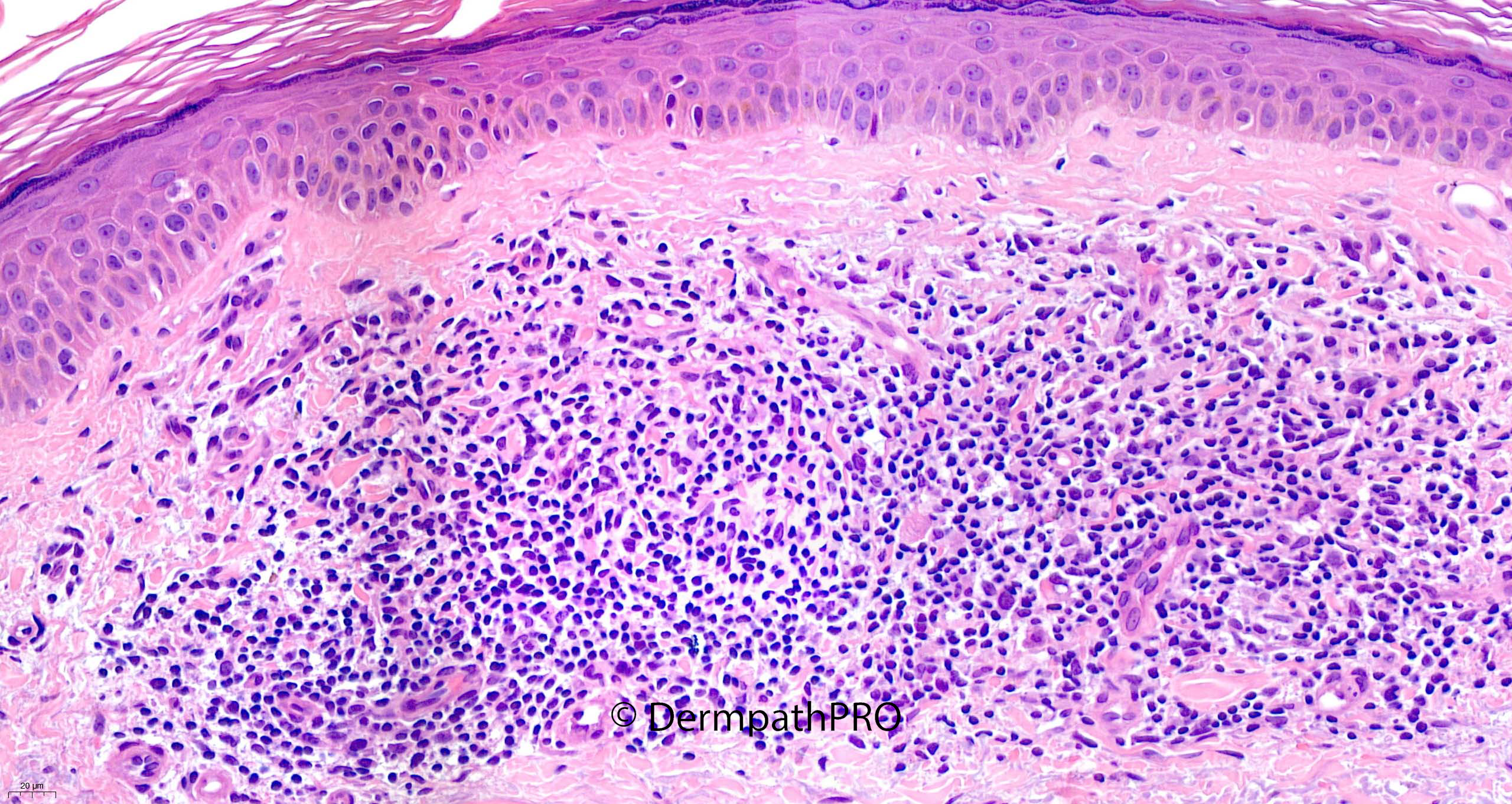
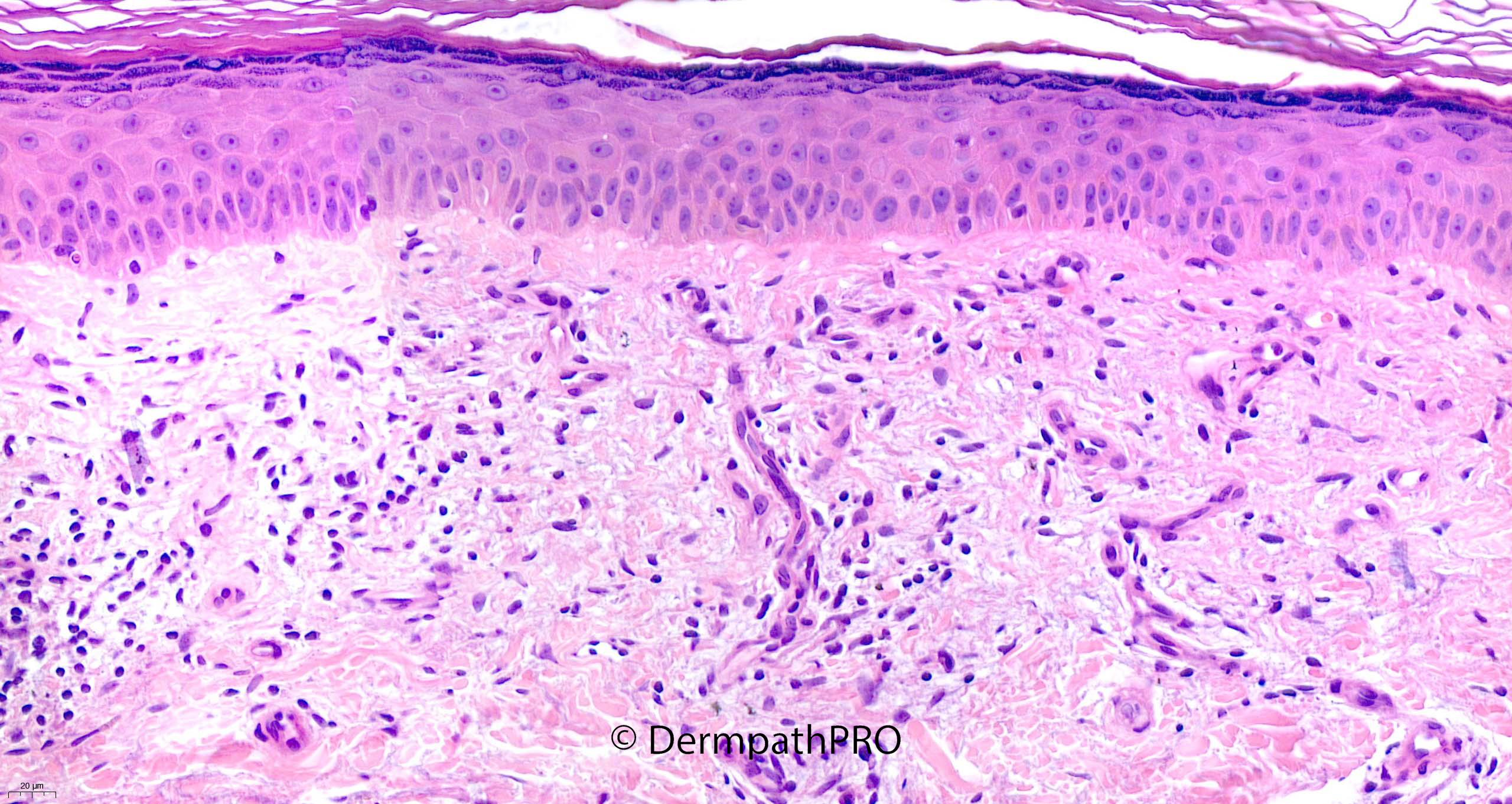
58F Punch biopsy right leg ?seborrhoeic keratosis ?BCC
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.