Diagnostic Pearls : Case 2936 - 07 October 2021
62F punch excision on nose ?BCC (previous history of melanoma on the back several years ago)
Saleem Taibjee
Posted 06/10/21
Posted 06/10/21
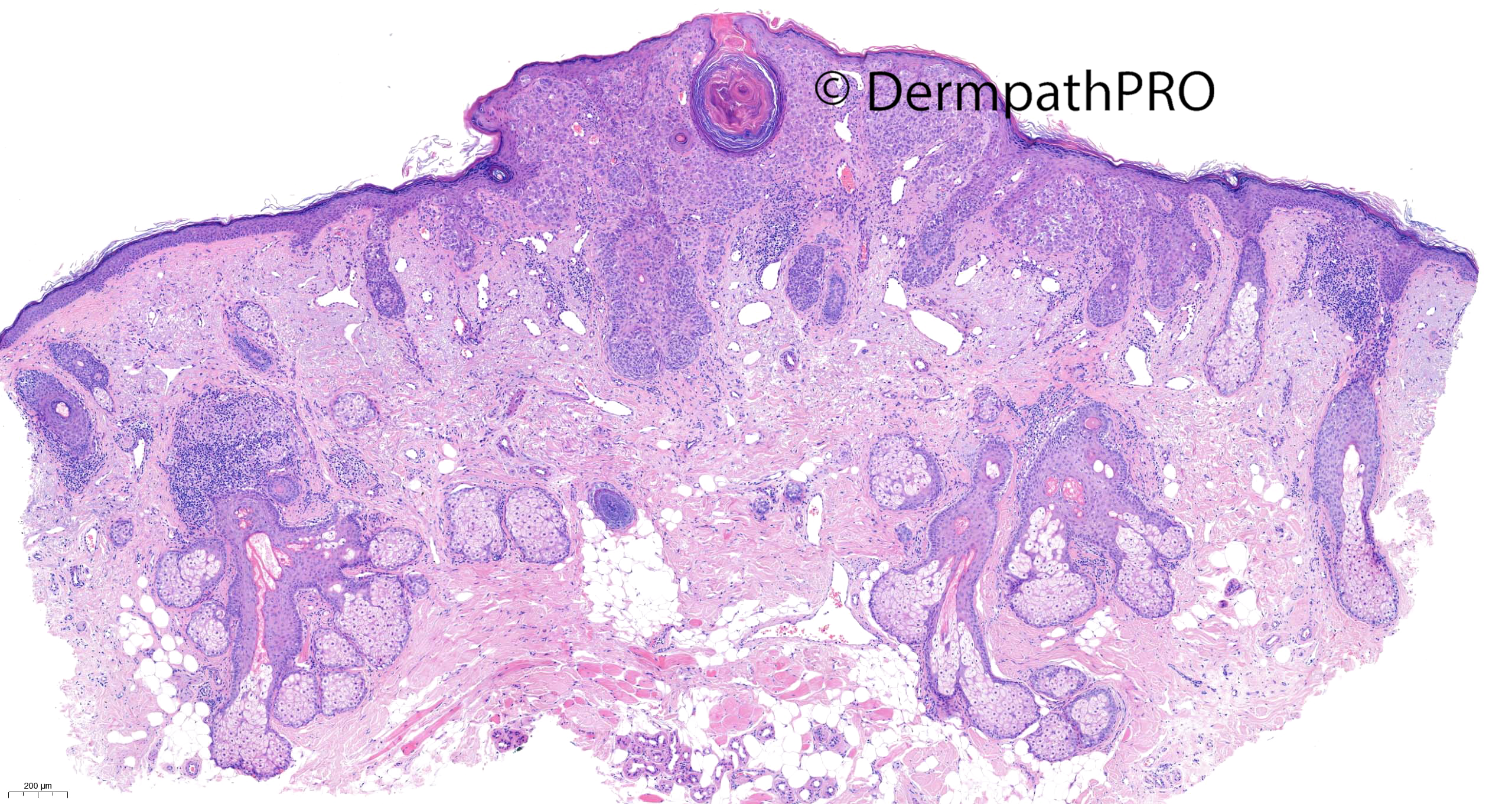
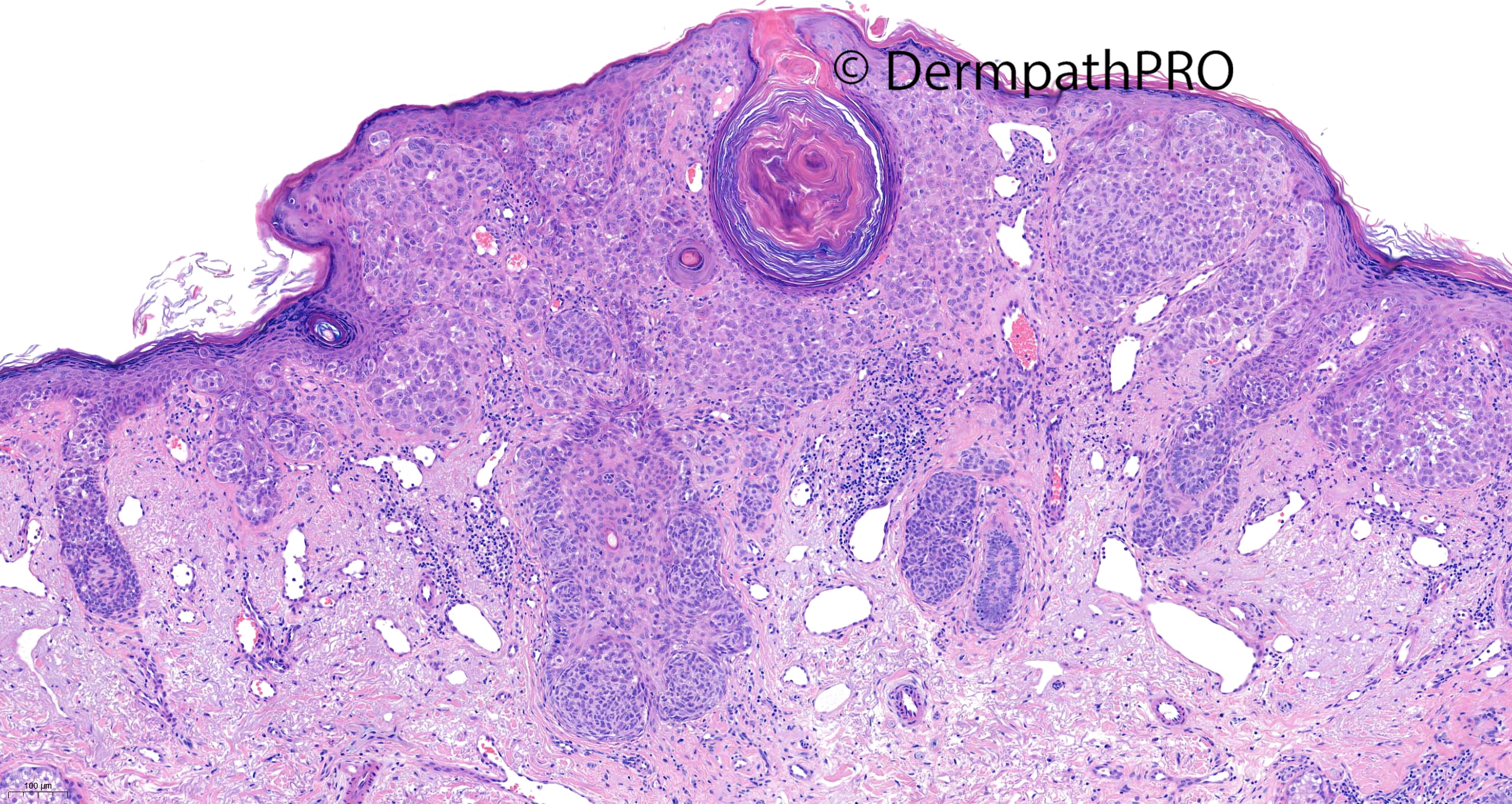
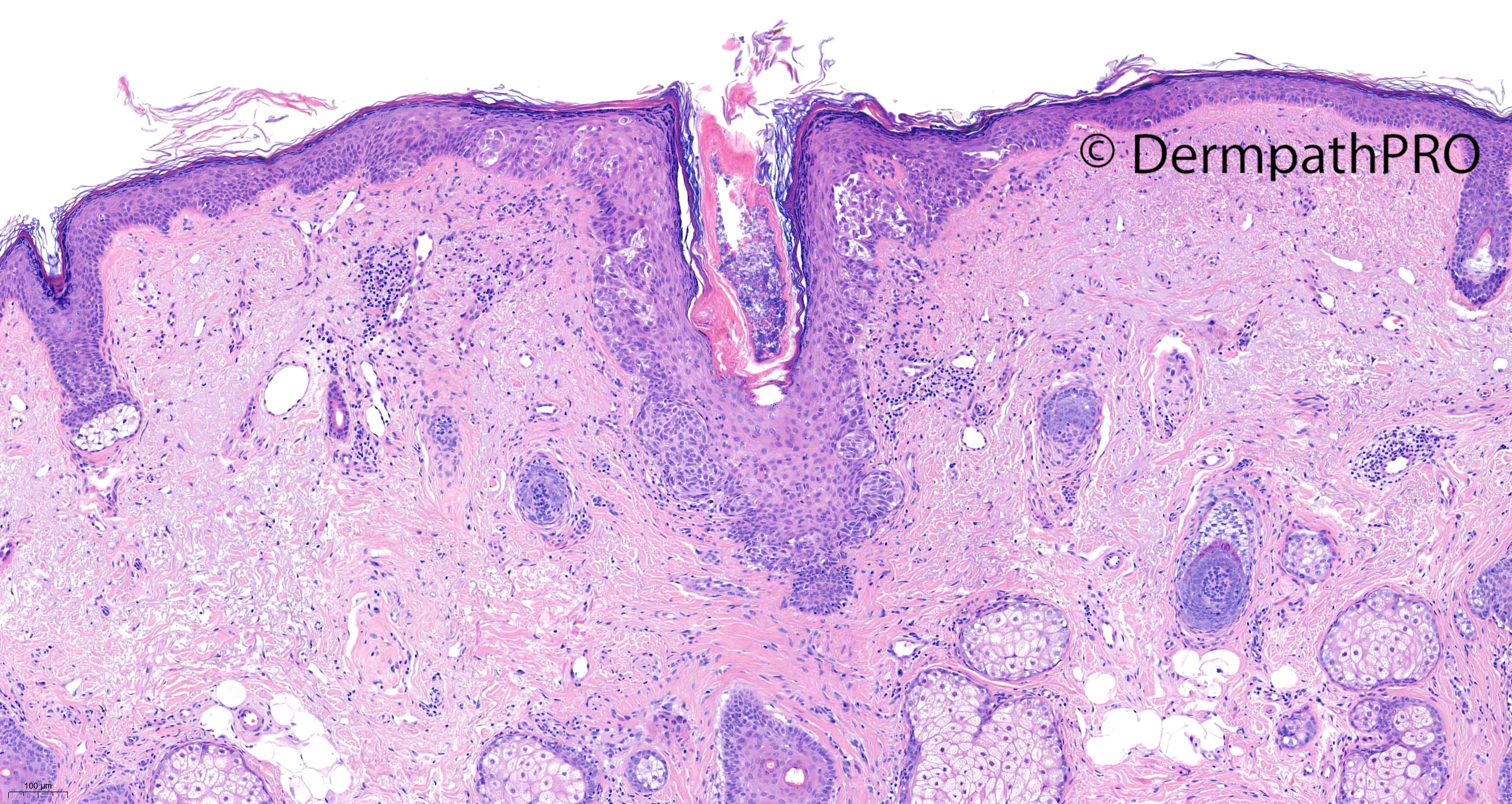
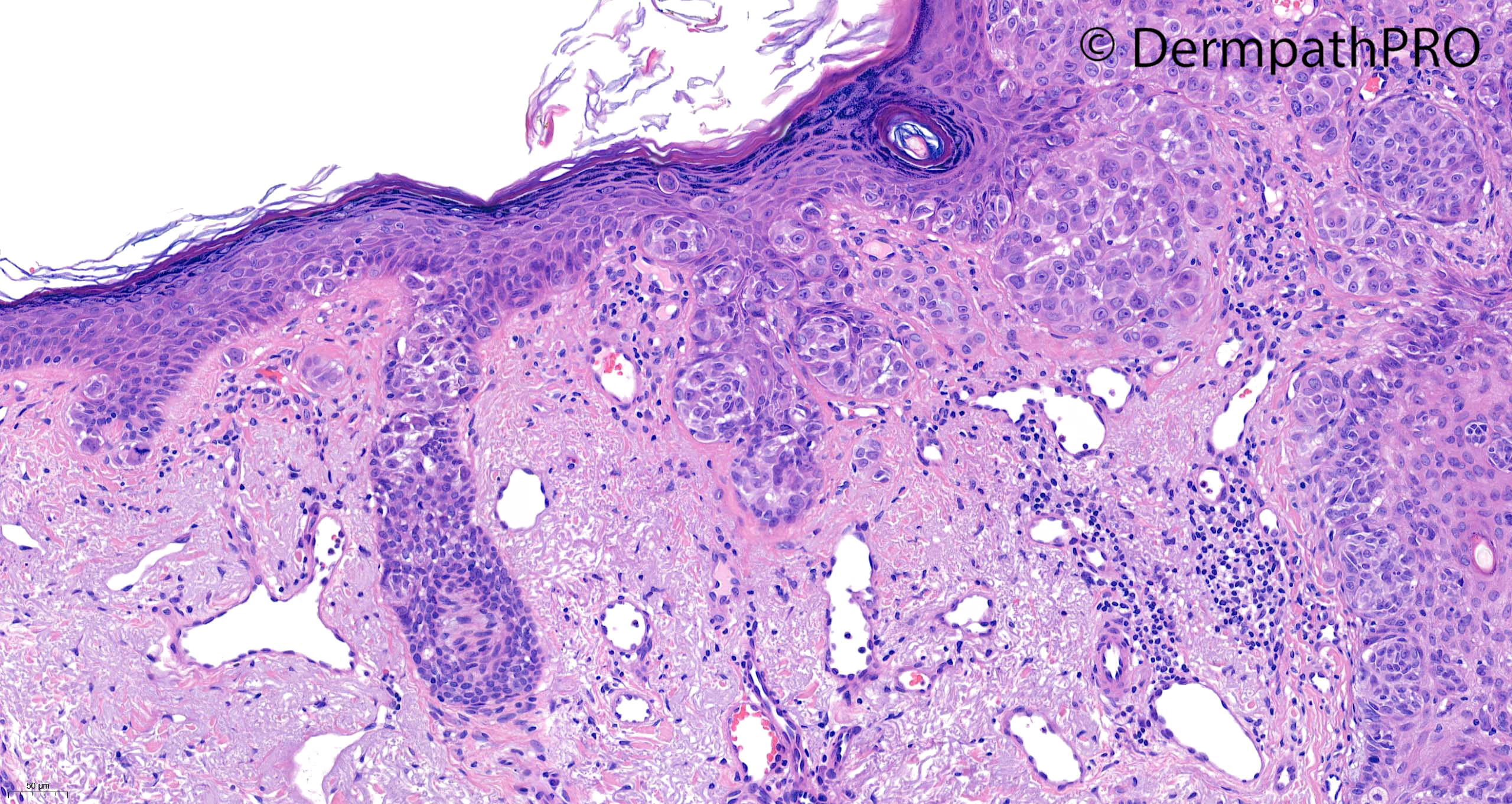
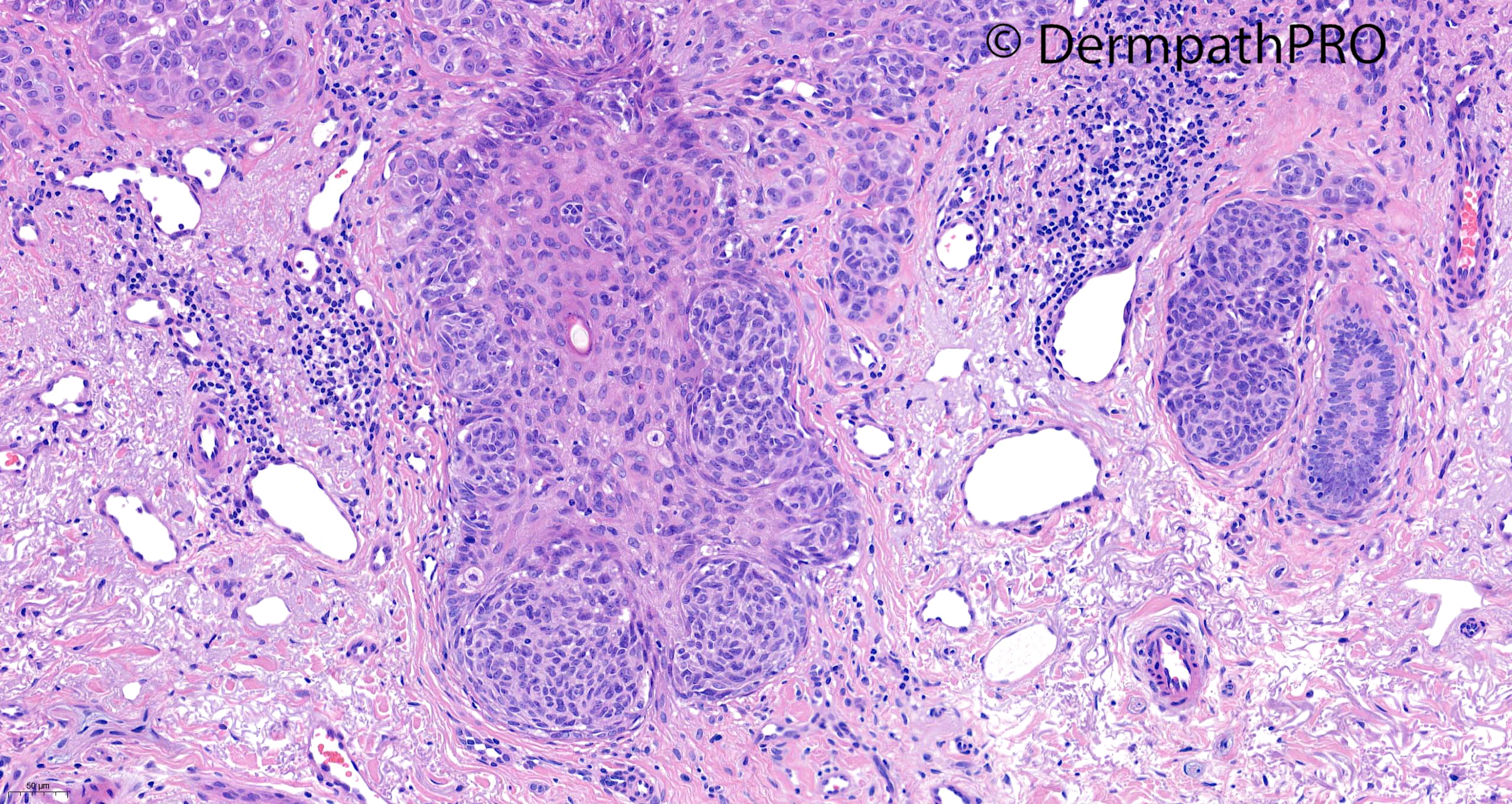
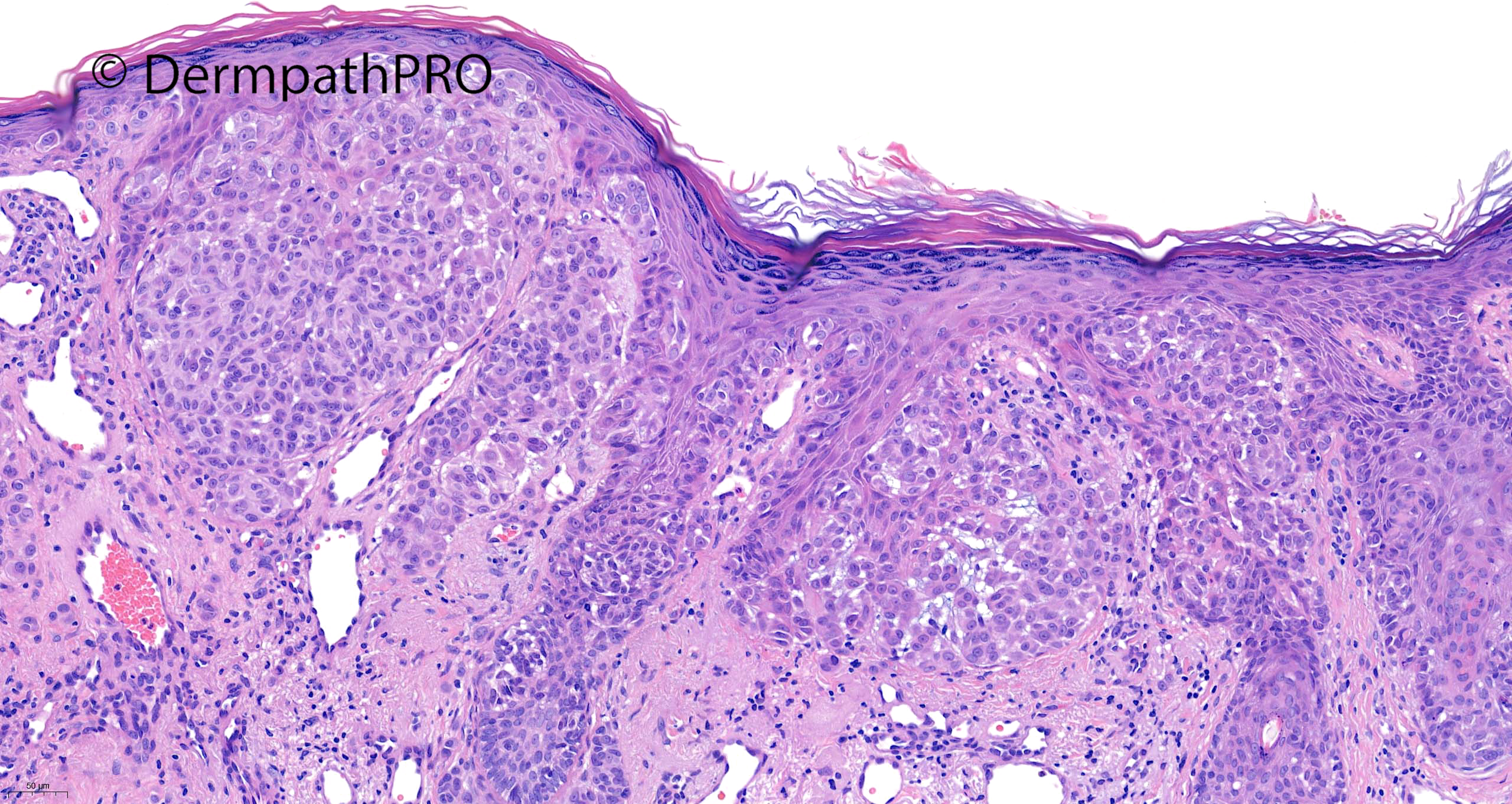
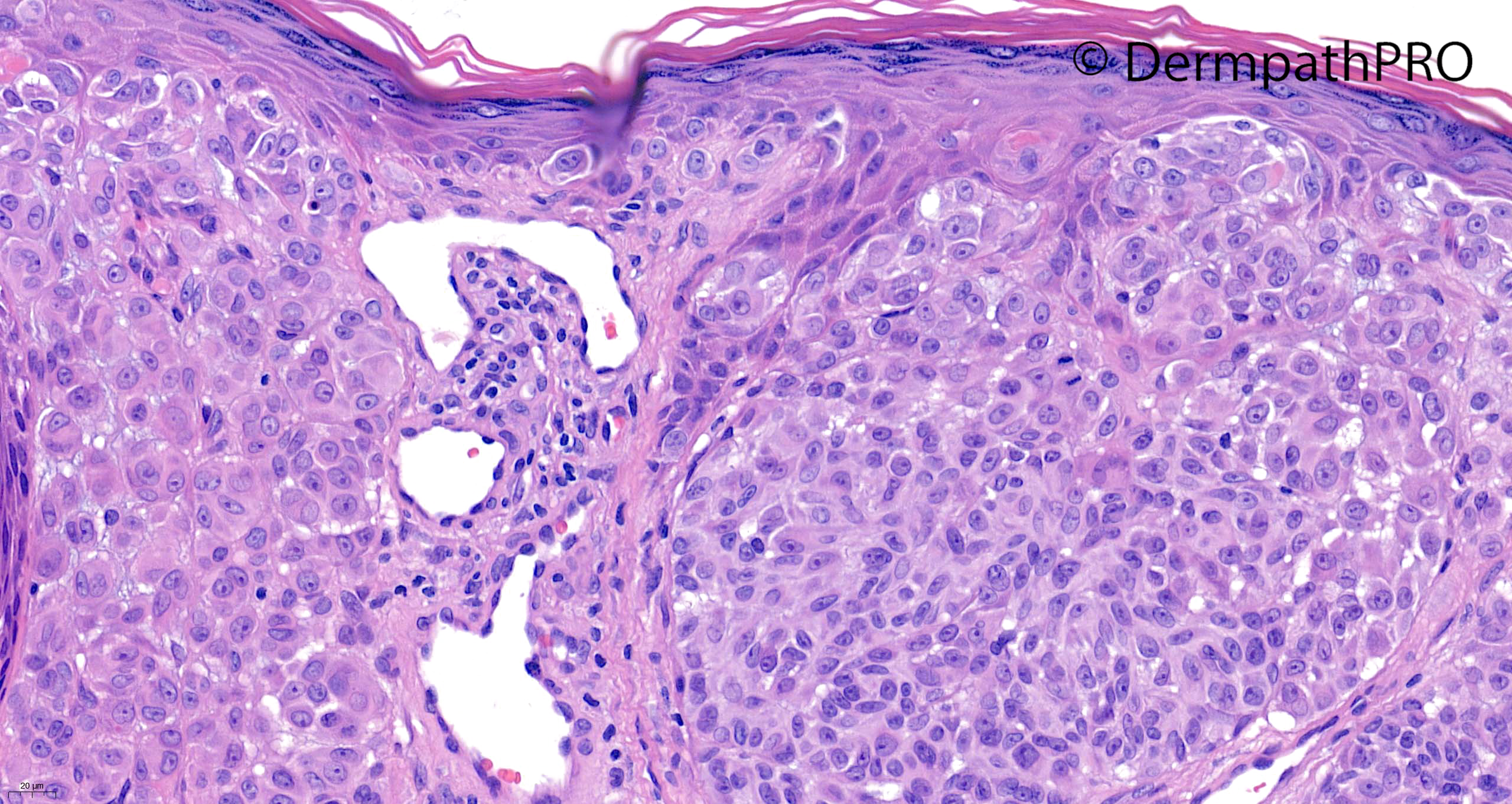
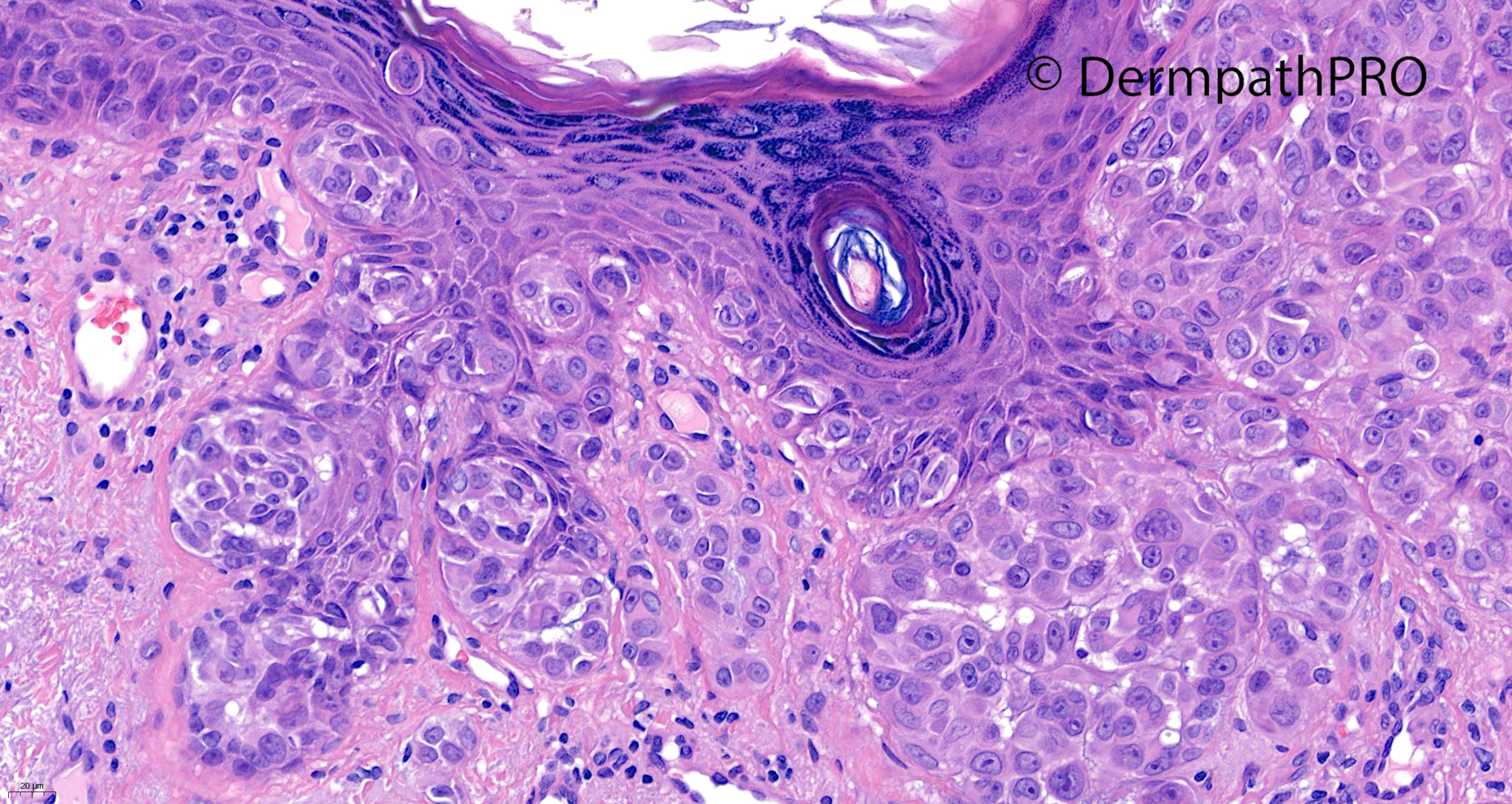
62F punch excision on nose ?BCC (previous history of melanoma on the back several years ago)
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.