Diagnostic Pearls : Case 4156 - 26 December 2022
F 45 with SLE, Disseminated pustular rash
Dr.Mona Abdel-Halim
Posted 26/12/22
Posted 26/12/22
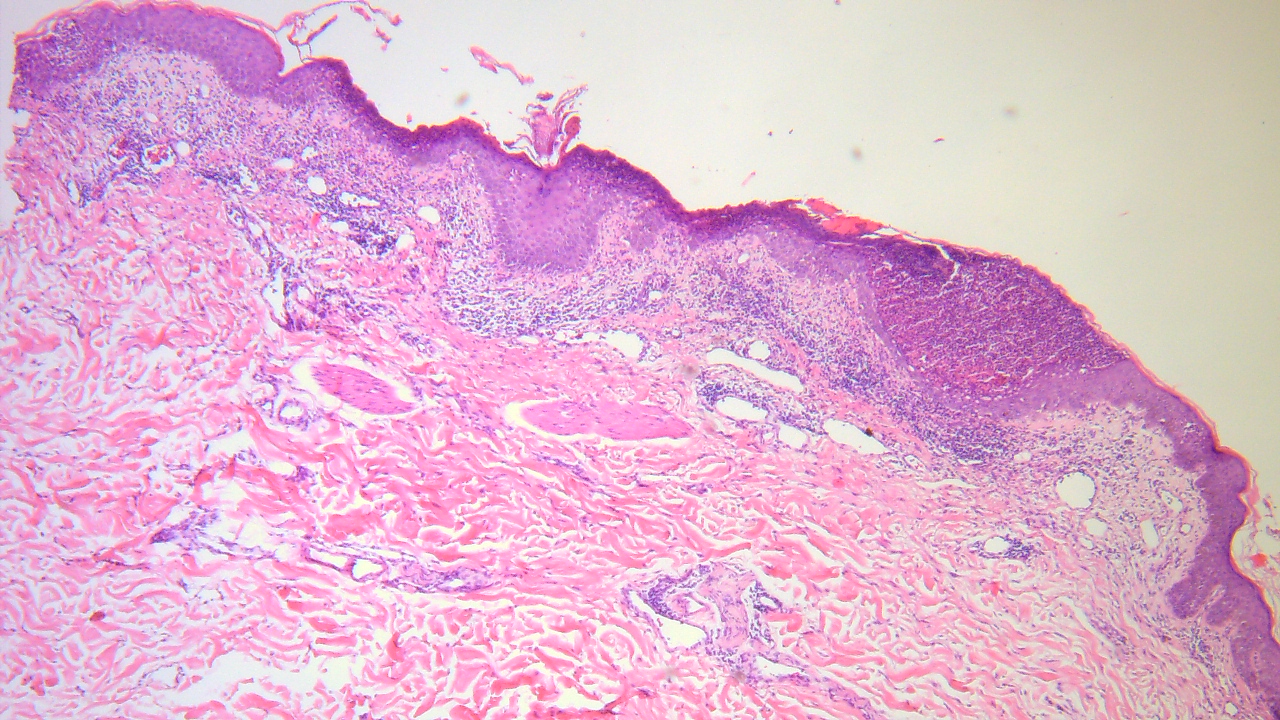
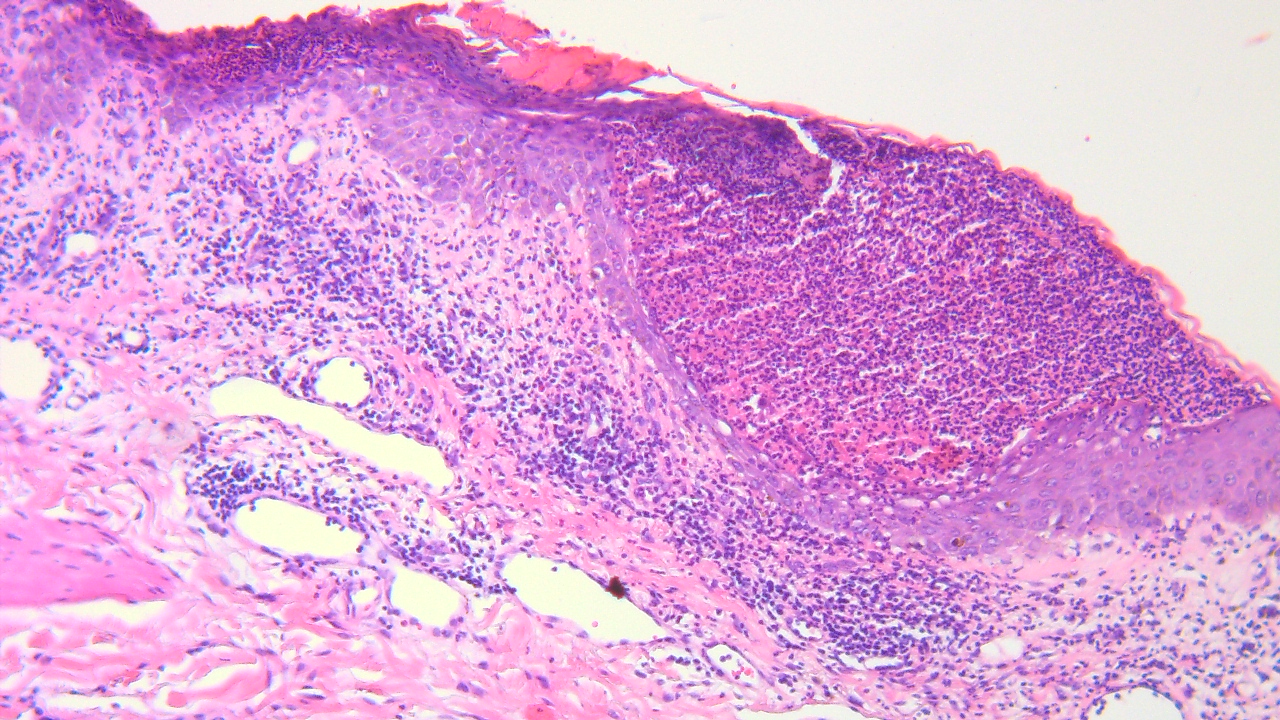
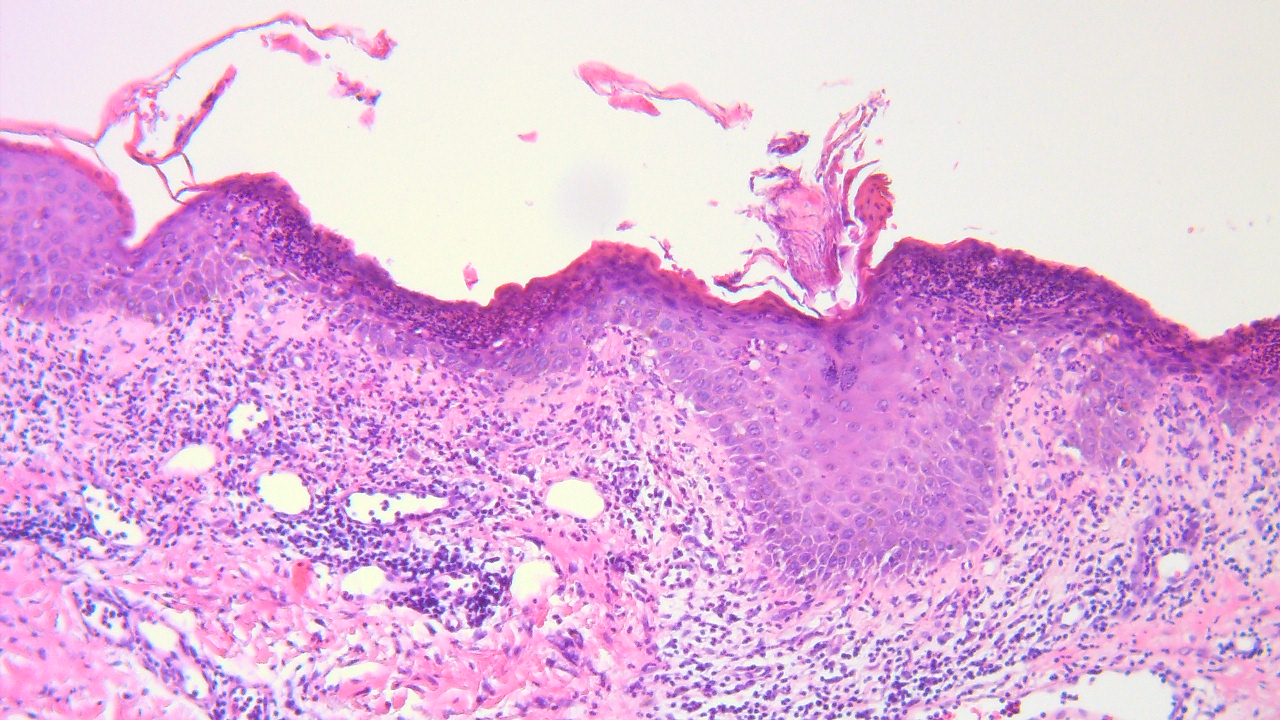
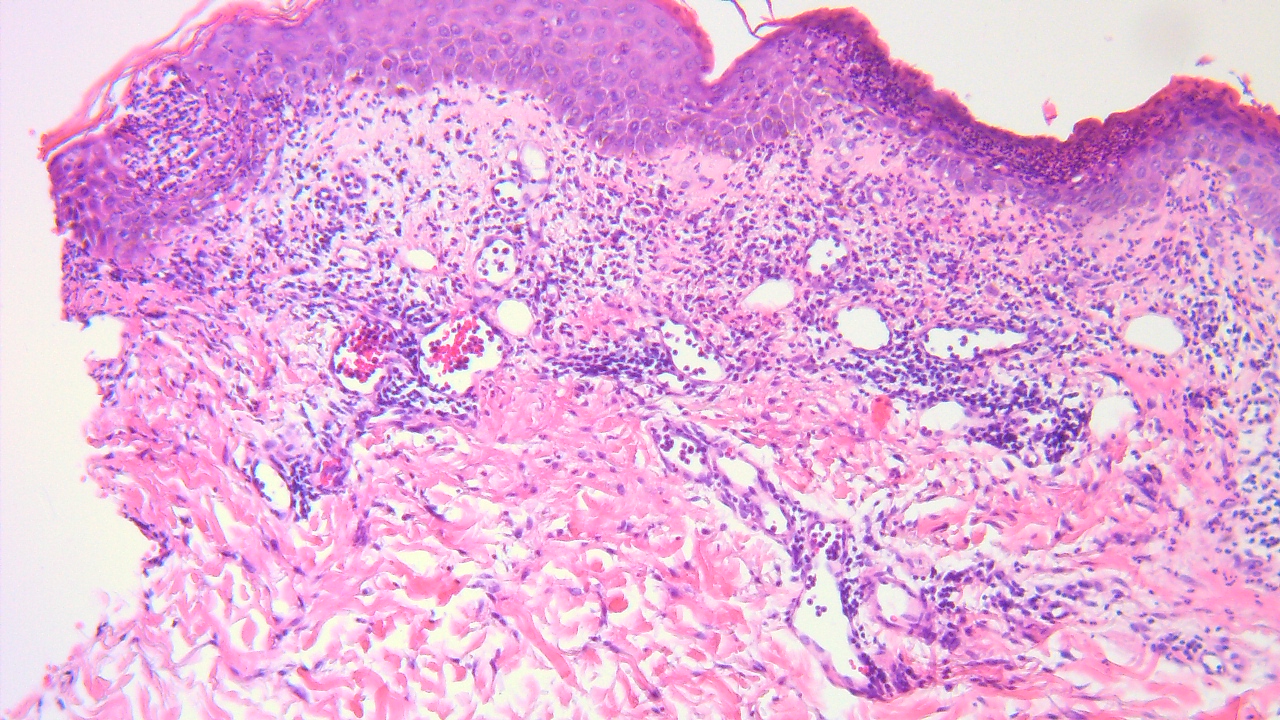
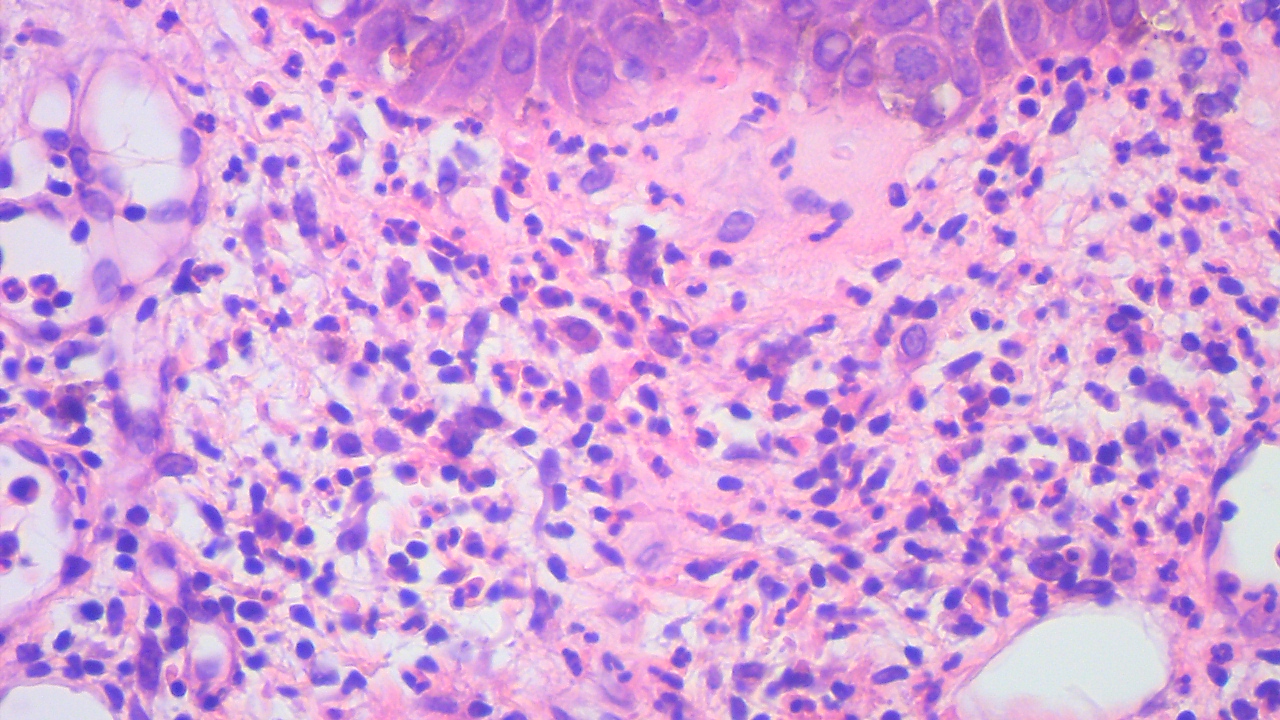
F 45 with SLE, Disseminated pustular rash
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.