Diagnostic Pearls : Case 3022 - 4 February 2022
M85. Scalp Vertex. 4 months nodule ?SCC ?BCC
Dr. Richard Carr
Posted 03/02/22
Posted 03/02/22
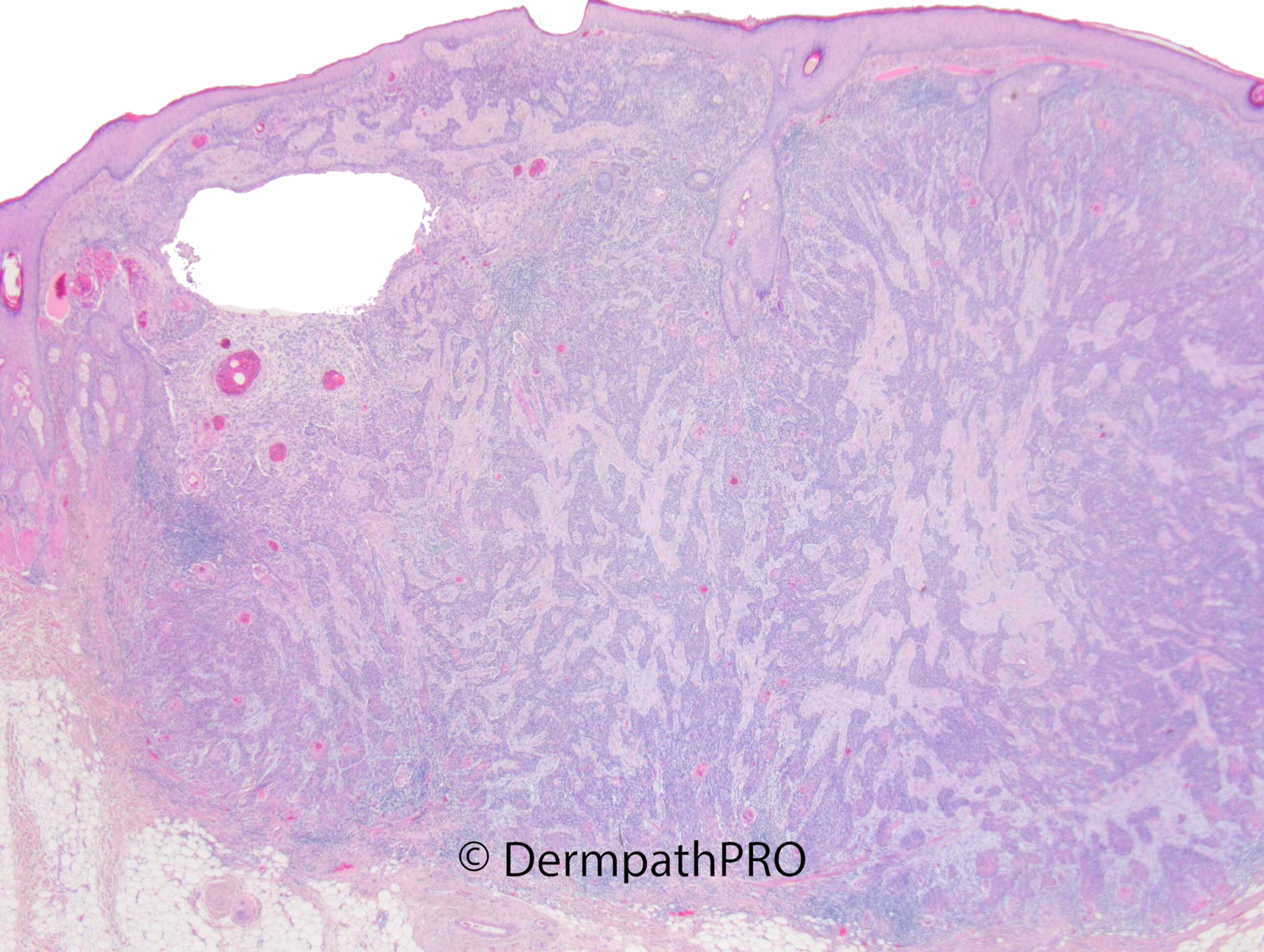
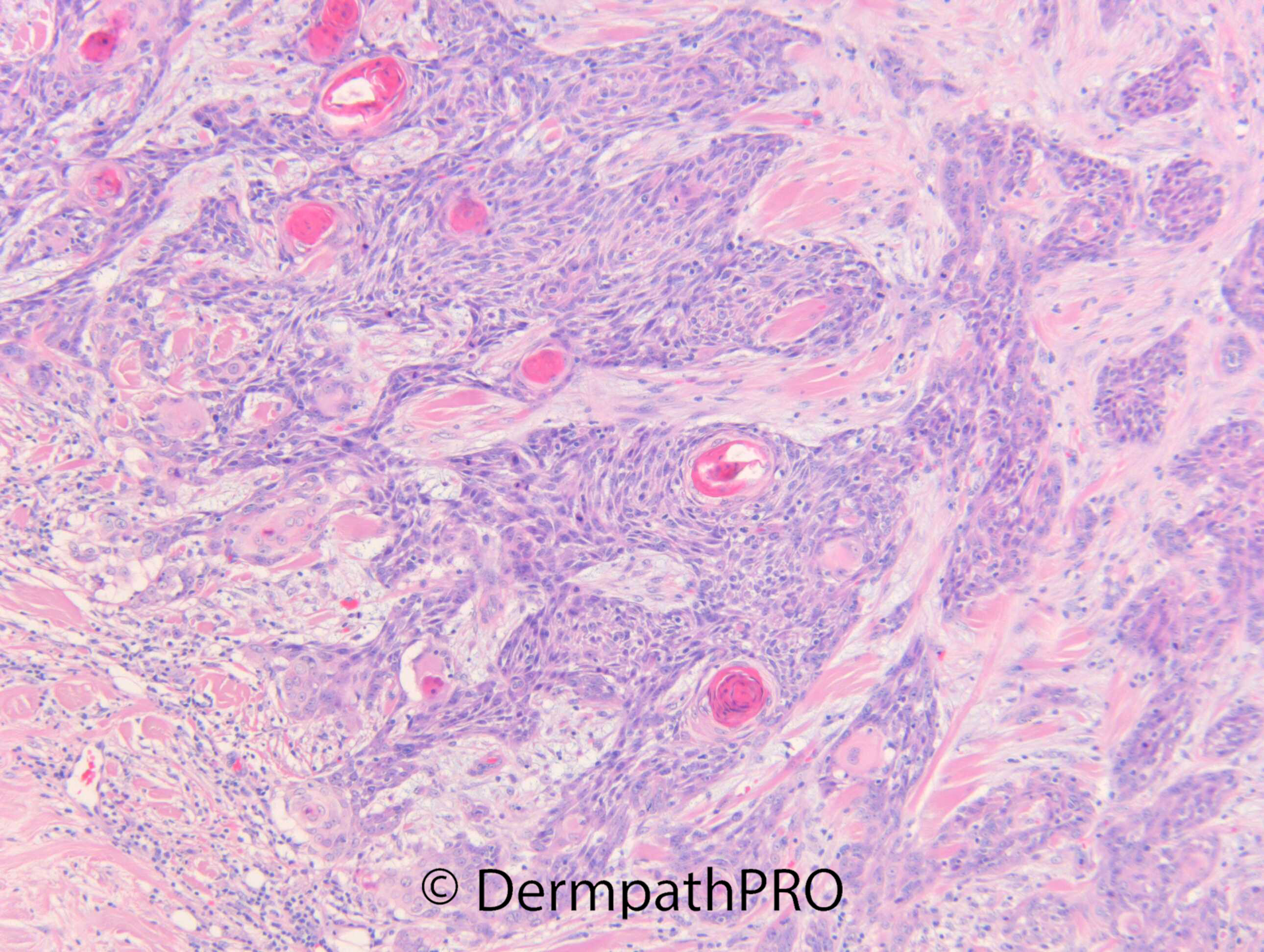
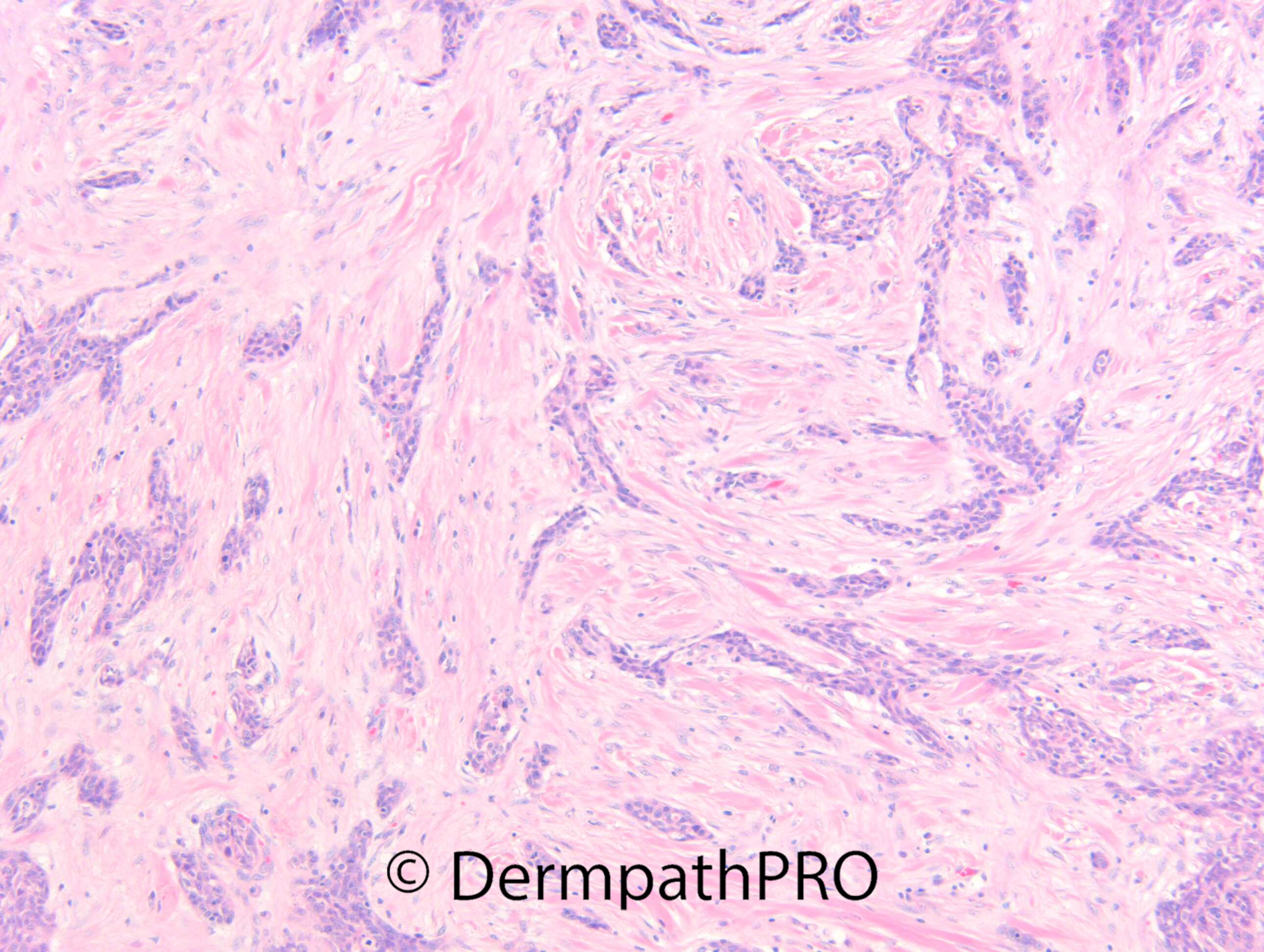
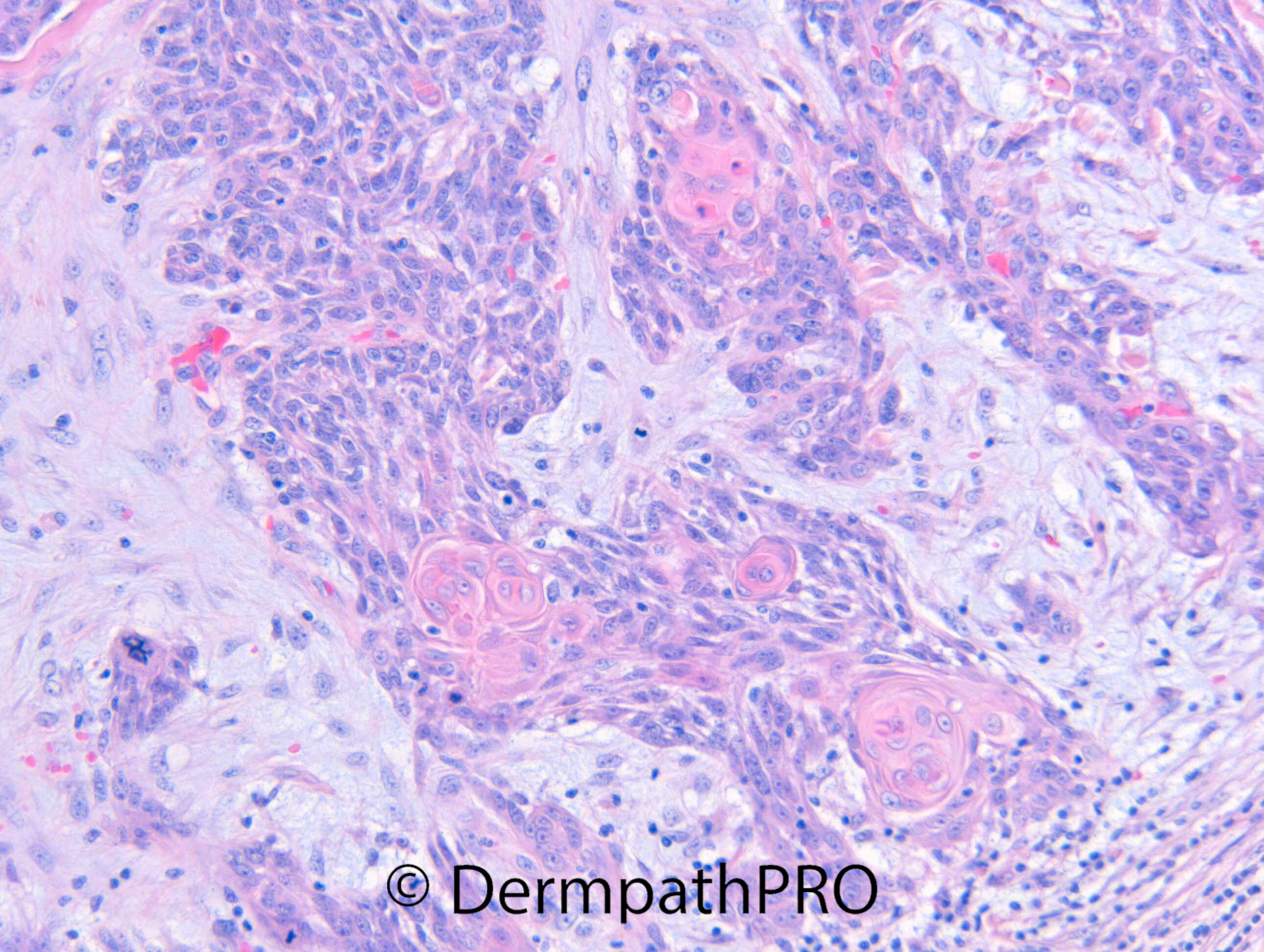
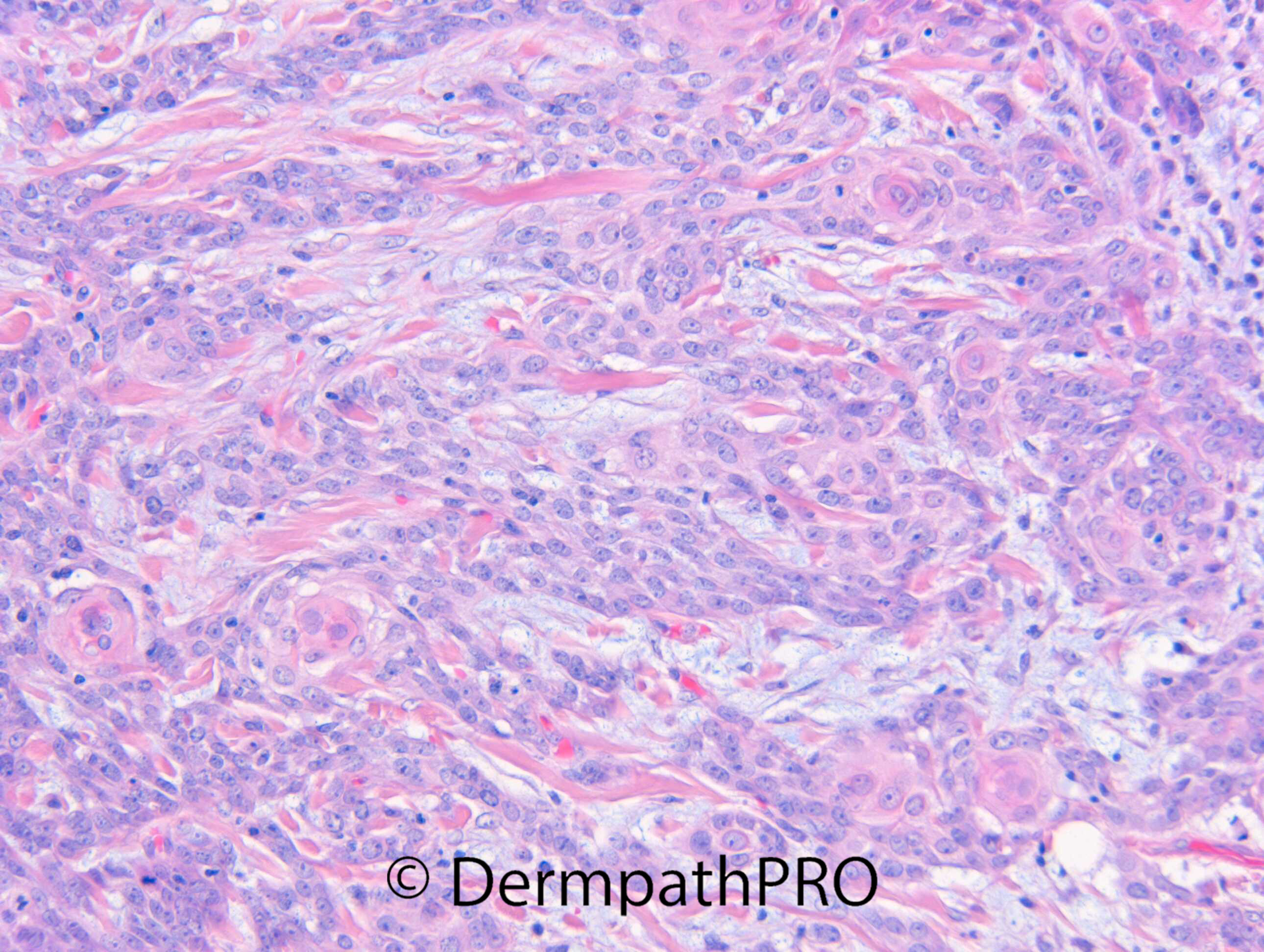
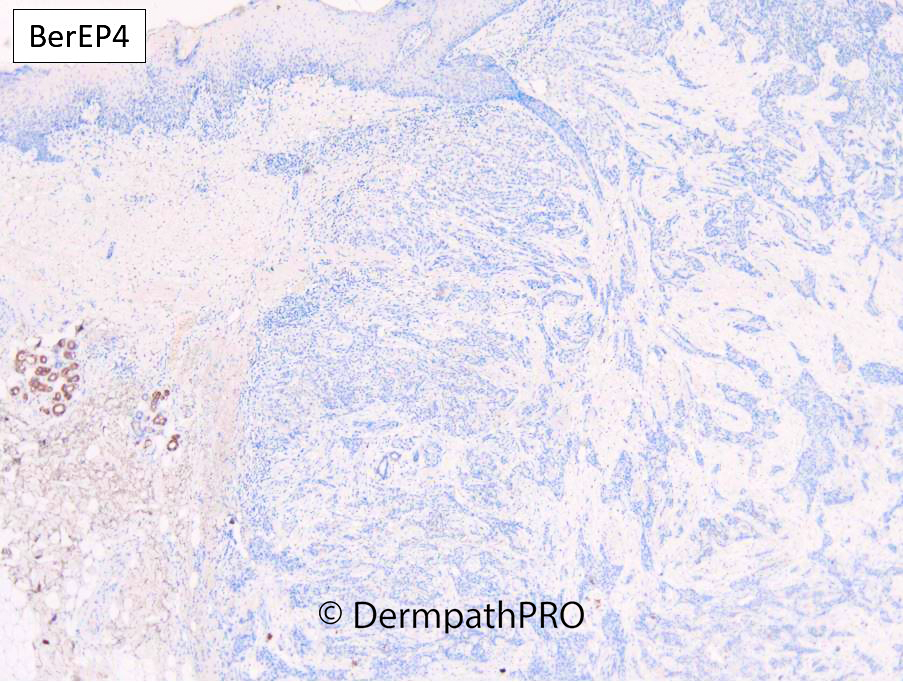
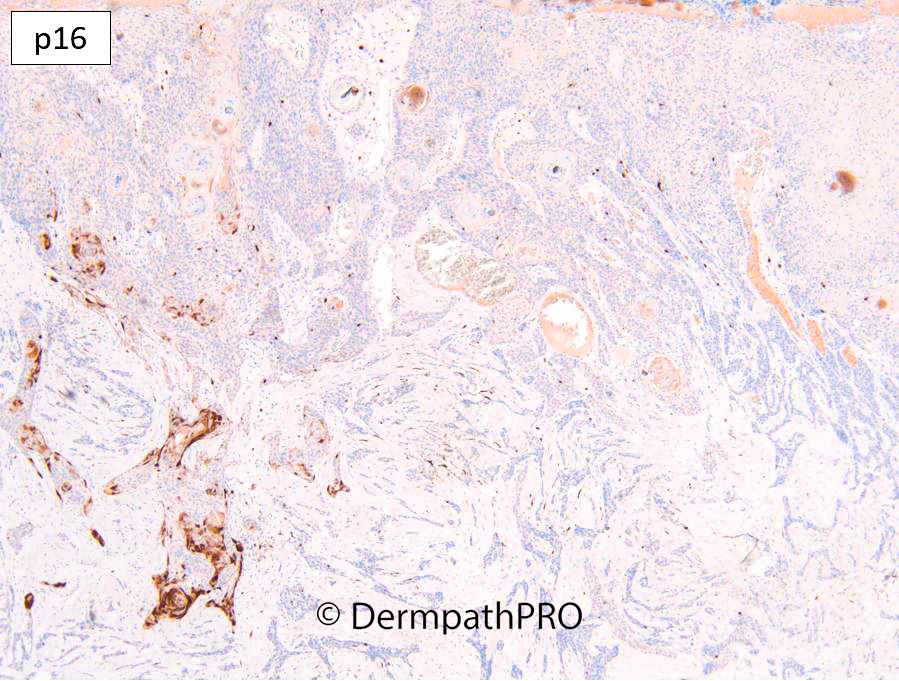
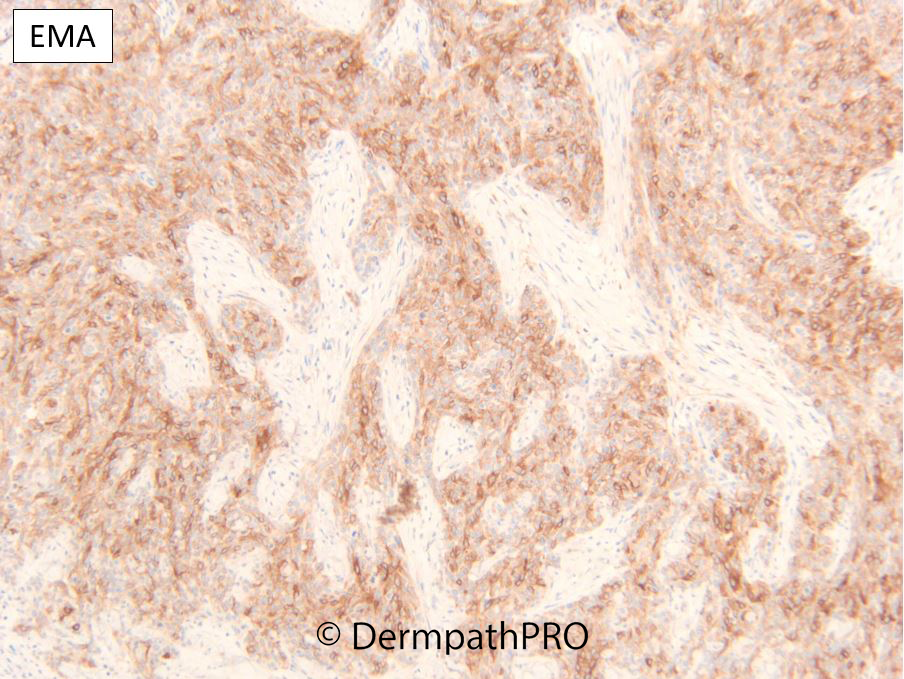
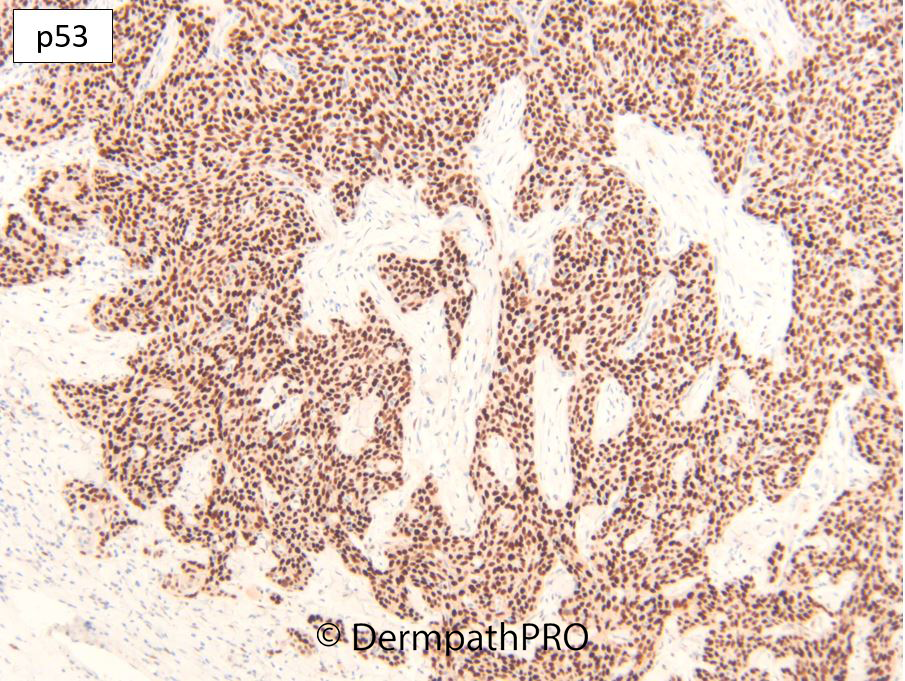
M85. Scalp Vertex. 4 months nodule ?SCC ?BCC
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.