Diagnostic Pearls : Case 3052 - 18 March 2022
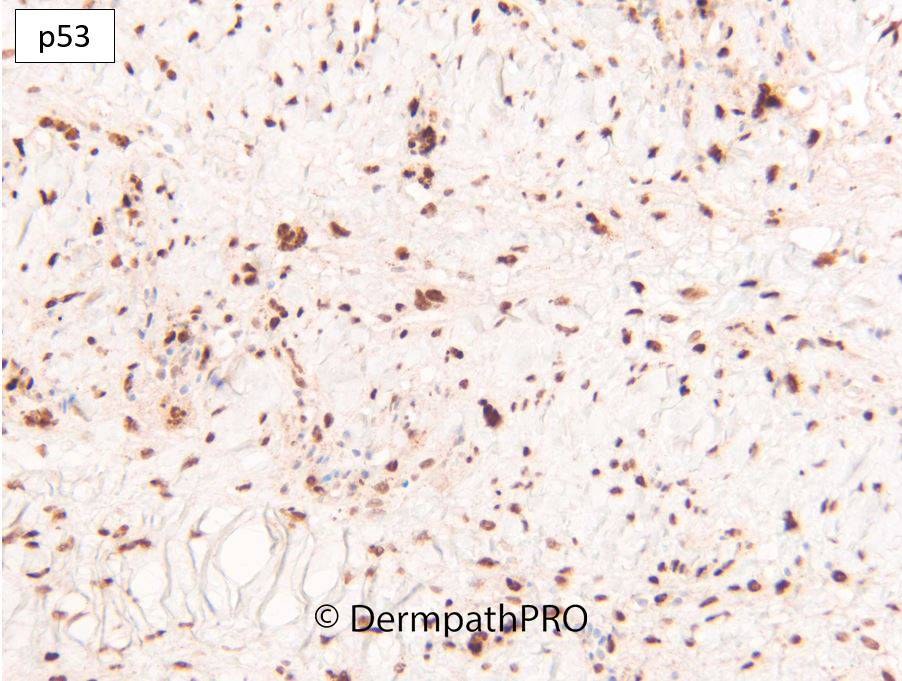
M75. Vertex scalp. 10mm purple lesion, incidental finding. ?BAK, ?angiosarcoma, ?AFX
Dr. Richard Carr
Posted 17/03/22
Posted 17/03/22
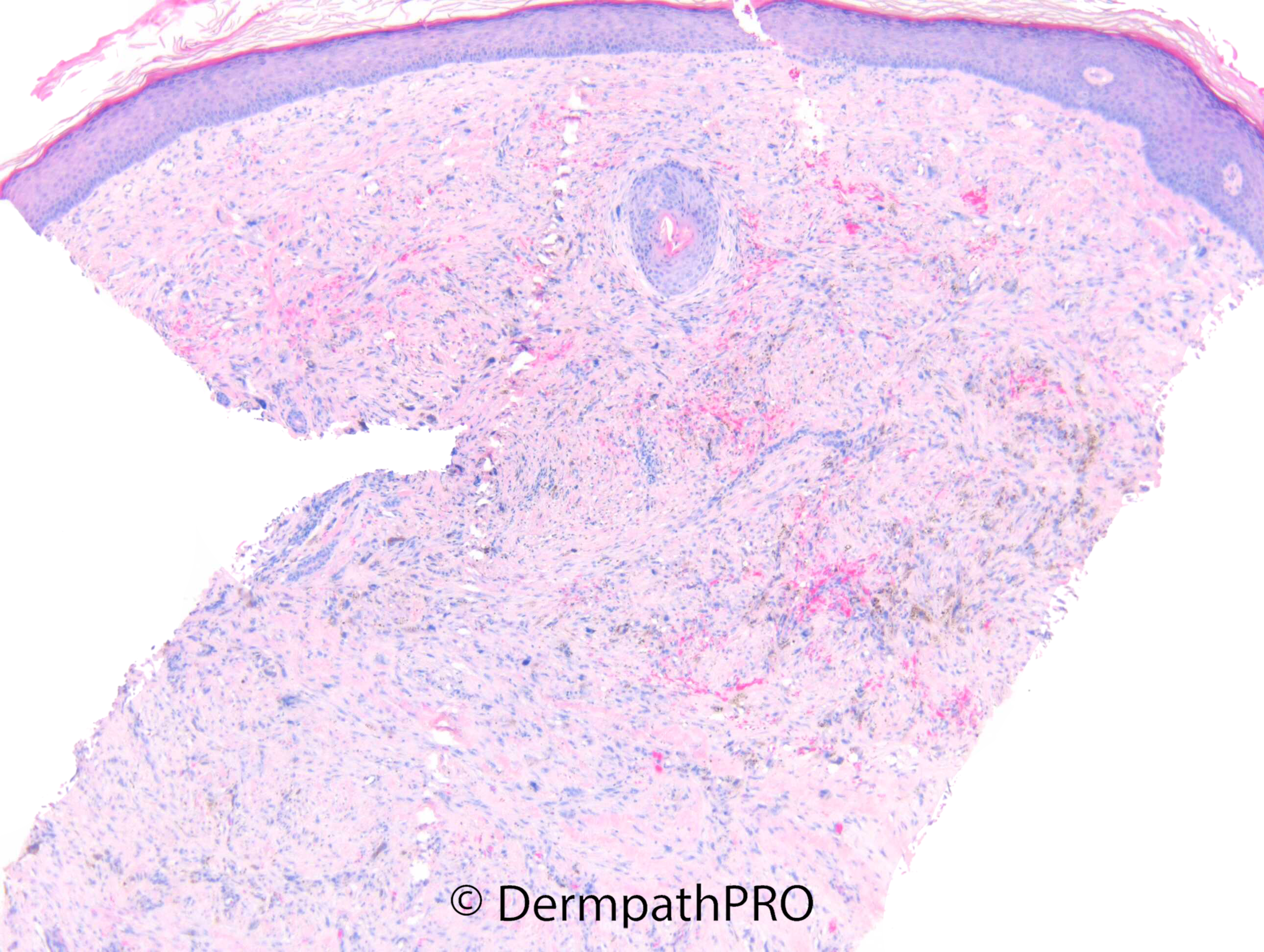
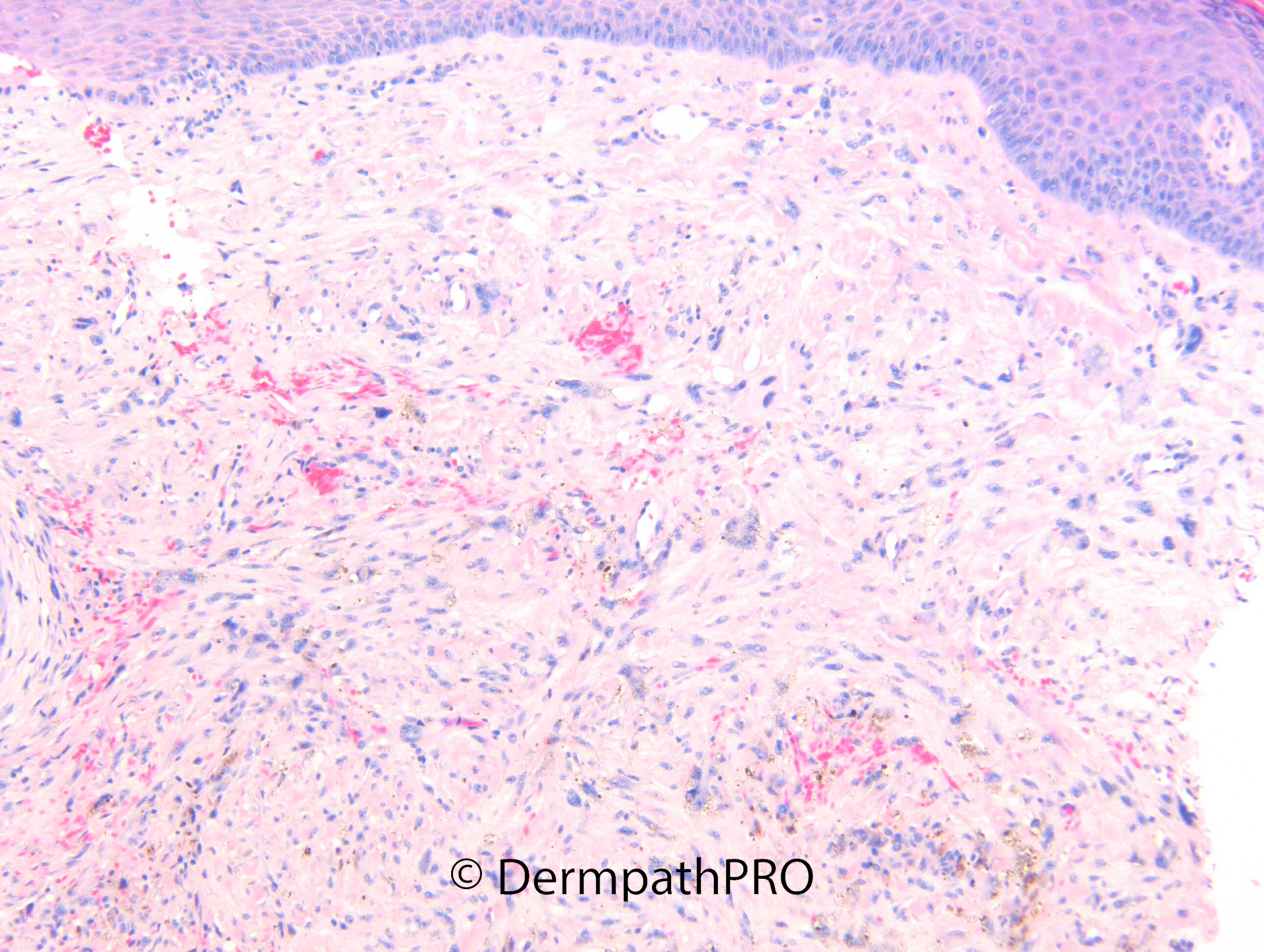
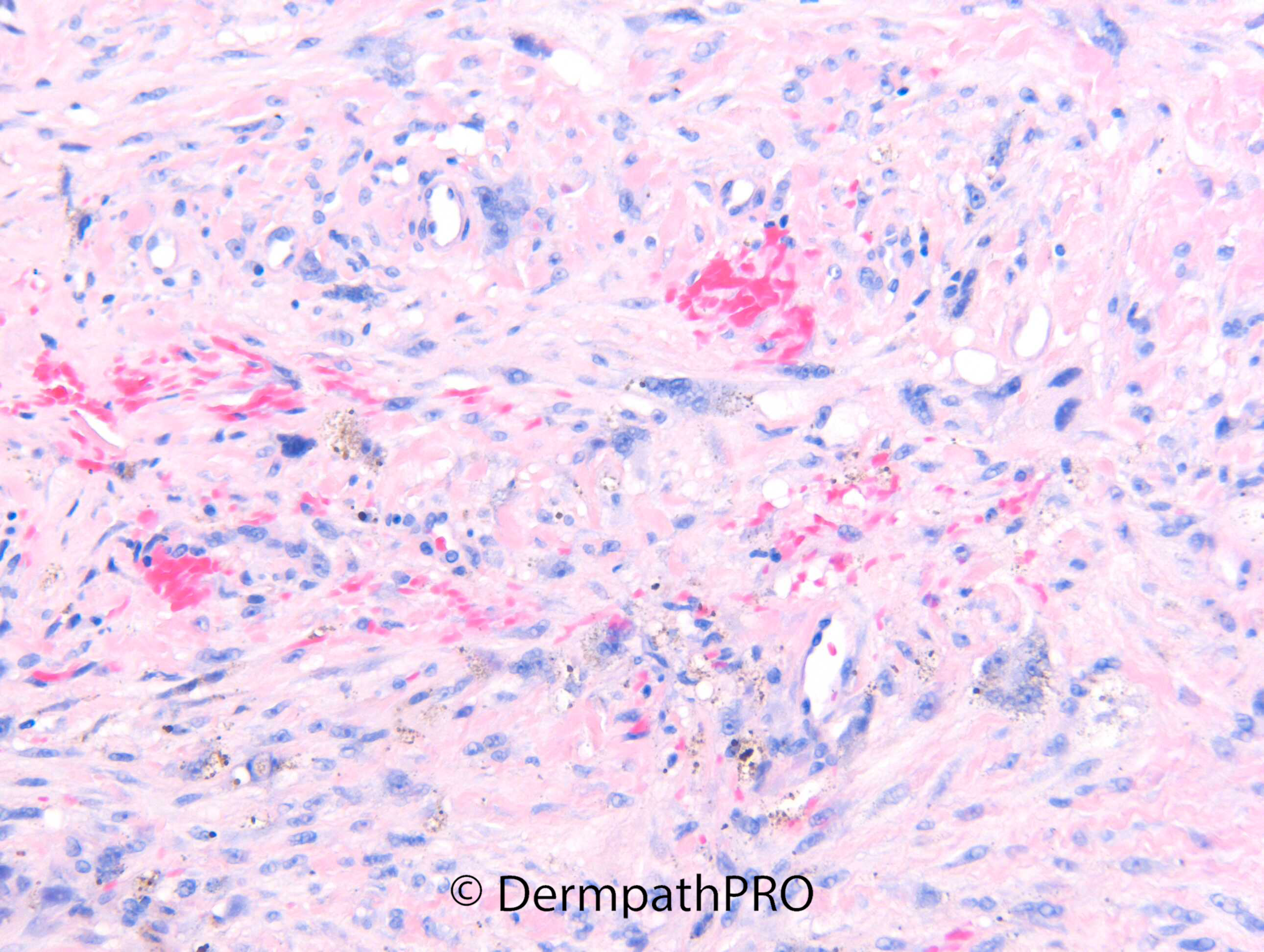
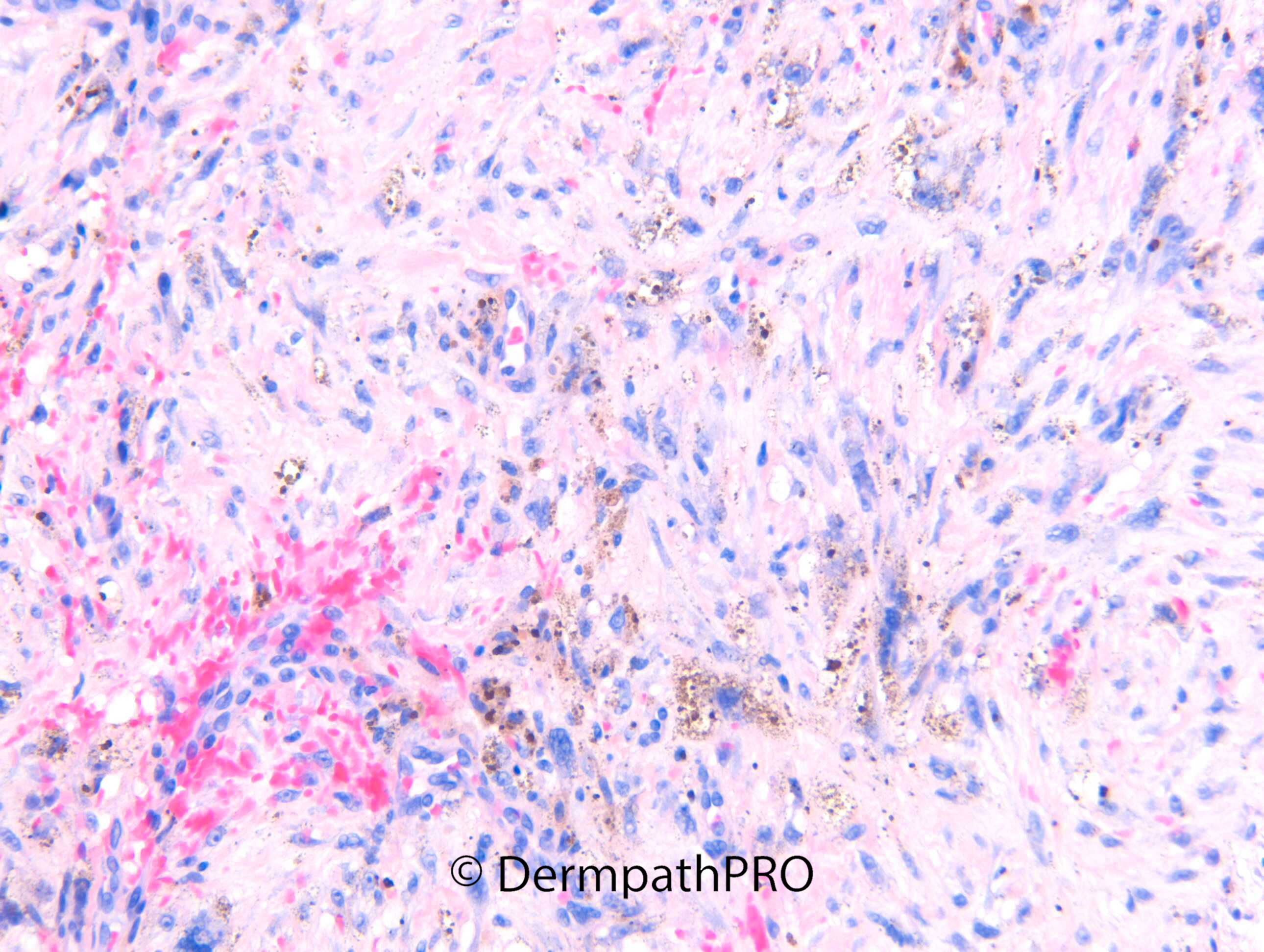
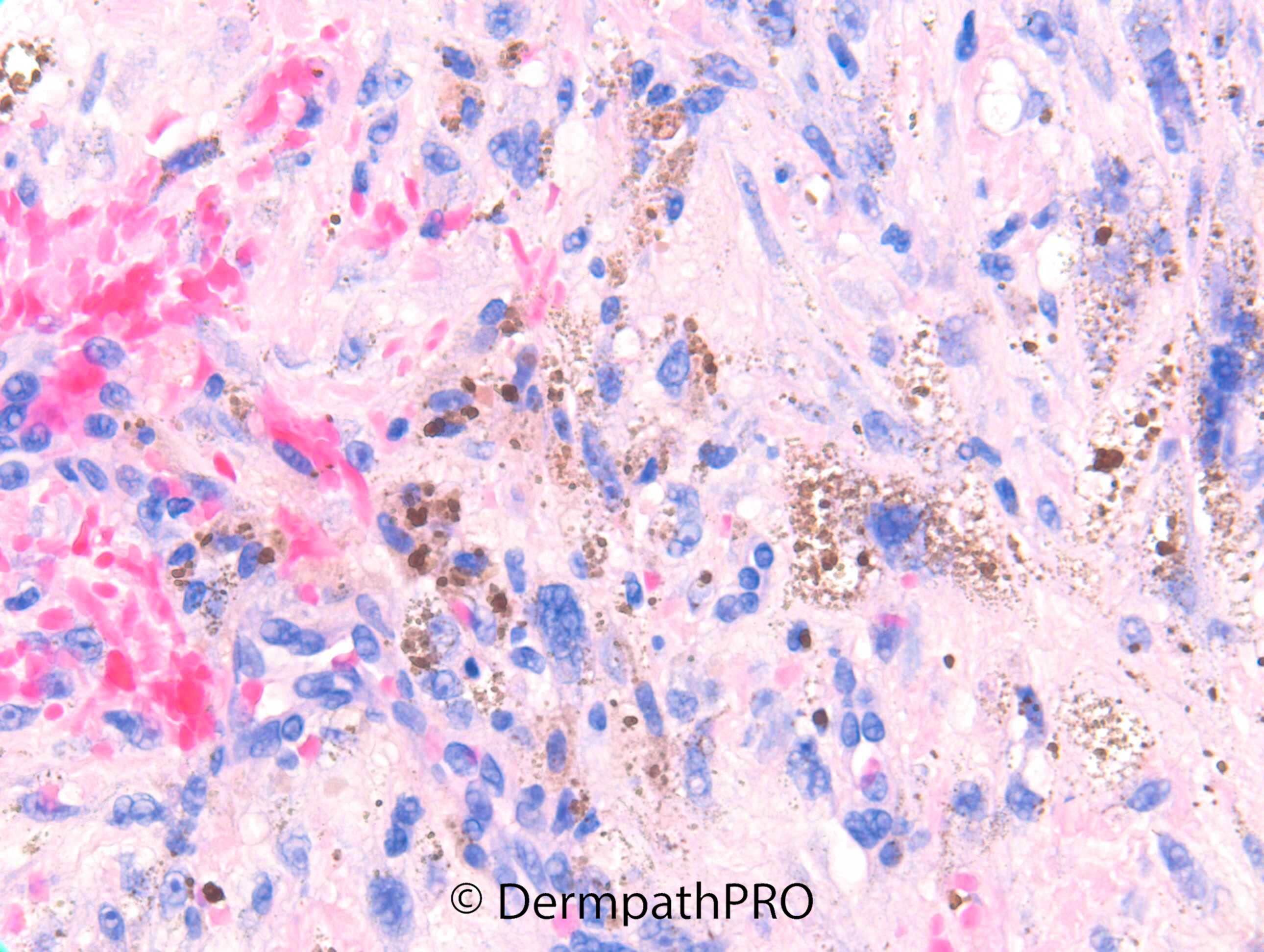
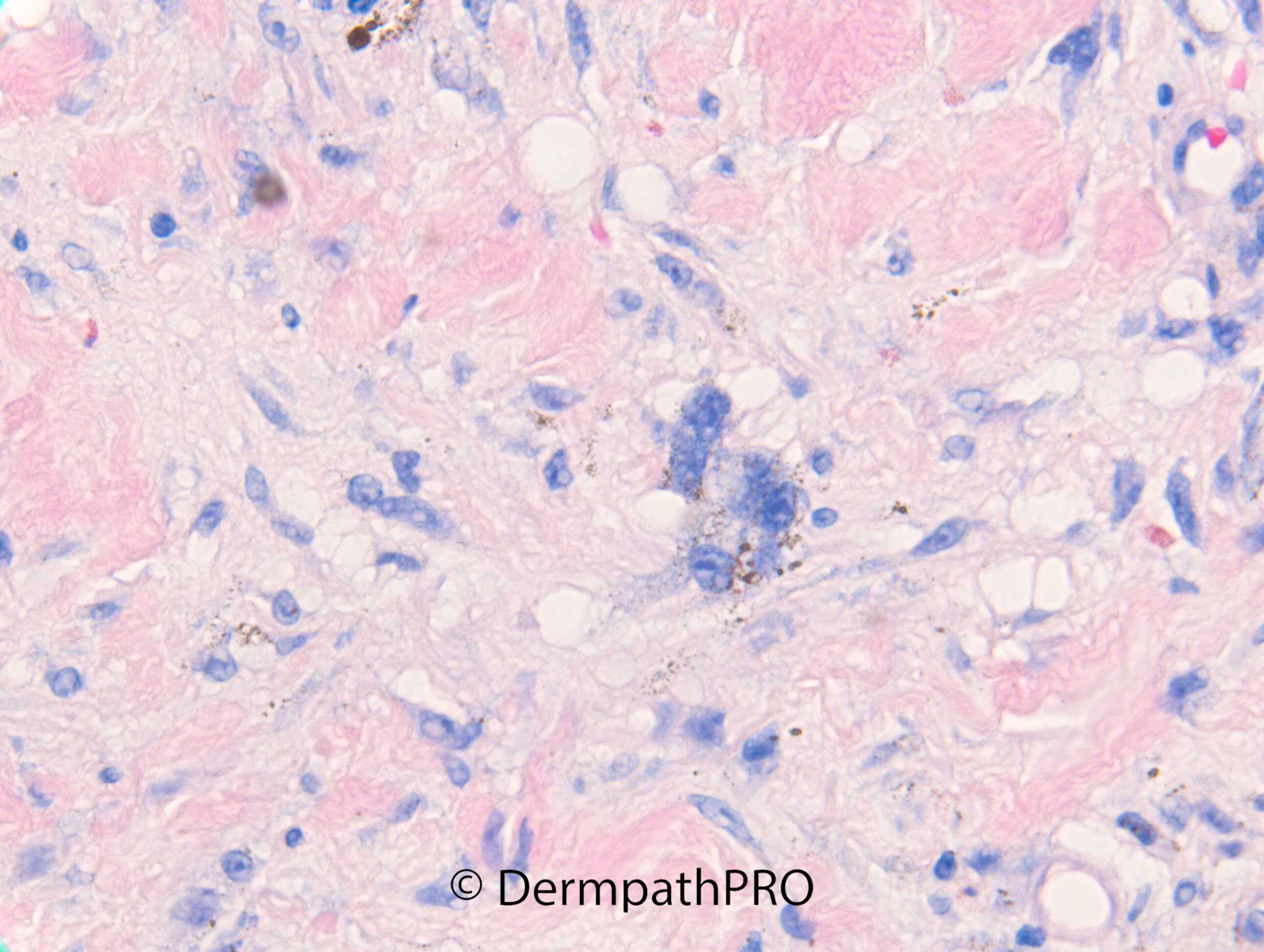
M75. Vertex scalp. 10mm purple lesion, incidental finding. ?BAK, ?angiosarcoma, ?AFX
Join the conversation
You can post now and register later. If you have an account, sign in now to post with your account.